Reduction of Deviation Angle During Occlusion Therapy: In Partially Accommodative Esotropia with Moderate Amblyopia
Article information
Abstract
Purpose
To evaluate changes in ocular alignment in partially accommodative esotropic children age ranged from 3 to 8 years during occlusion therapy for amblyopia.
Methods
Angle measurements of twenty-two partially accommodative esotropic patients with moderate amblyopia were evaluated before and at 2 years after occlusion therapy.
Results
Mean deviation angle with glasses at the start of occlusion treatment was 19.45±5.97 PD and decreased to 12.14±12.96 PD at 2 years after occlusion therapy (p<0.01). After occlusion therapy, 9 (41%) cases were indications of surgery for residual deviation but if we had planned surgery before occlusion treatment, 18 (82%) of patients would have had surgery. There was a statistical relationship between increase of visual acuity ratio and decrease of deviation angle (r=-0.479, p=0.024).
Conclusions
There was a significant reduction of deviation angle of partially accommodative esotropic patients at 2 years after occlusion therapy. Our results suggest that occlusion therapy has an influence on ocular alignment in partially accommodative esotropic patients with amblyopia.
An esotropia is partially accommodative when accommodative factors contribute to but do not account for the entire deviation.1 In most instances the deviation is probably congenital with an accommodative element becoming superimposed as the child grows older, but in other cases a nonaccommodative element develops after initial alignment of the eyes with glasses as form of decompensated accommodative esotropia if the treatment is delayed. The mainstay of treatment is a full correction of hypermetropic refractive error and a surgery for the residual deviation. And the initiation of amblyopia treatment before surgical correction of strabismus is recommended in current clinical guidelines.2
However, there has been considerable disagreement regarding the effect of occlusion therapy on the amount of preexisting esodeviation. If there is the possibility of changes in the deviation with the occlusion therapy, this raise important question about the proper timing and the amount of surgery of partially accommodative esotropic patients with amblyopia.
The aim of the present study is to evaluate changes of ocular alignment in partially accommodative esotropic patients with moderate amblyopia during occlusion therapy.
Materials and Methods
The medical records were reviewed from 59 patients with a diagnosis of partially accommodative esotropia and amblyopia who had undergone occlusion therapy. There are 8 inclusion criteria for this retrospective study. These parameters were: (1) having hypermetropia ≥ 1.5D (some cases were included if there was any decrease in esodeviation after full correction of patient's hypermetropia less than 1.5D), (2) presence of manifest deviation after full correction of refractive error for at least 2 months, (3) their age at the start of occlusion treatment ranged from 3 to 8 years, (4) presence of moderate amblyopia which include three to five lines acuity difference,3 (5) had not been treated with occlusion before and had no previous eye muscle surgery, (6) no evidence of central nervous system abnormalities or anatomic abnormalities of the eye, (7) no evidence of dissociated vertical deviation or dysfunction of oblique muscles, (8) their follow-up periods at least 2 years.
And 22 patients fulfilled these inclusion criteria. The following parameters were reviewed and analyzed: age, gender, spherical equivalents of refractive errors, age at onset of strabismus, age at the start of therapy, duration of occlusion therapy, visual acuities and manifest deviations before and at 2 years after occlusion therapy and length of follow-up.
All patients in this study had a complete ophthalmologic examination prior to treatment by authors. A cycloplegic refraction was performed using 1% cyclopentolate and 0.5% tropicamide at the first visit and then glasses correcting their full refractive errors were prescribed. The angle of deviation was measured at 6 and 0.33 m by alternate prism cover test, if not possible, by Krimsky methods at each visit. Visual acuities were measured by Snellen's chart or 'E' chart. Visual acuities were compared by calculating the visual acuity ratio which is the ratio of the Snellen acuity of the amblyopic eye with the Snellen acuity of the sound eye. The visual acuity ratio allows an estimate of the magnitude of the amblyopia and permits direct comparison of changes in the amount of amblyopia between visits of the same patients and between patients.4
Initial occlusion durations were half of awakened hours (2~6 hr) and duration of occlusion and frequencies of visits were determined according to the response to occlusion therapy and patients' compliance. After occlusion therapy, patients were considered as surgical indications if they still have near manifest deviation with glasses more than 15 PD.
Near manifest deviation angles with glasses and visual acuity ratios before and at 2 years of follow-up were compared with Wilcoxon signed rank test. To investigate the possible correlation between visual acuity improvement and the change of deviation angle, Spearman's correlation coefficient was calculated. To compare clinical characteristics of surgical and non-surgical group, Mann-Whitney U test was used.
Results
Table 1 shows descriptive data of 22 patients in this study group. The age at the onset of treatment was significantly older than the age at onset of strabismus and this delay of diagnosis and treatment may be the cause of amblyopia and development of nonaccommodative deviation in patients of this study. Mean refractive error of the amblyopic eye at the onset of treatment was +2.76 D (+1.0 D~+7.5 D) and mean refractive error of the sound eye was +2.24D (+0.75 D~+7.0 D). There was no significant difference of refractive error between the amblyopic eye and the sound eye at the start of occlusion therapy (p=0.096). The occlusion treatment was performed 12.32±6.21 months of duration.
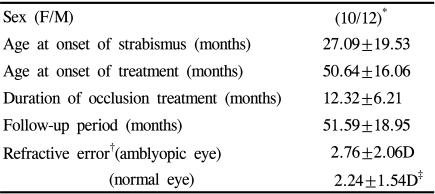
Patients data (Mean±SD)
During the occlusion therapy, a progressive and marked decrease in the nonaccommodative deviation angle was observed (Fig. 1). After 2 years of follow-up, mean manifest deviation angles with glasses was significantly decreased from 19.45±5.97 PD to 12.14±12.96 PD (p=0.003). Amblyopia was resolved in 15 (68%) patients.
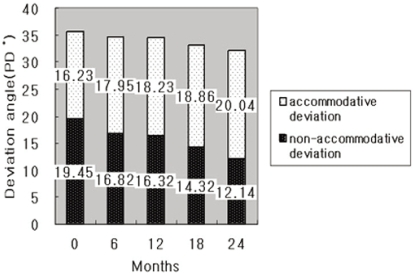
Changes of deviation angle during occlusion period.
PD*= prism diopter.
There was a remarkable improvement in the visual acuity ratio after occlusion therapy (p=0.0001). At the start of occlusion therapy, 18 patients (82%) had deviation within surgical limits (≥15 PD), but after occlusion treatment, only 9 patients (41%) of the patients were considered as surgical indications (p=0.003) (Table 2).

Deviation angles, visual acuity ratios and percentages of patients at the surgical limits prior to and after occlusion treatment. (Mean±SD)
Fig. 2 demonstrates the correlation between the amount of the increase of visual acuity ratio and the amount of the change of the deviation angle before and after 2 years of occlusion therapy. There was a statistically meaningful relationship between the increase of the visual acuity ratio and the decrease of the deviation angle. (r=-0.479, p=0.024)
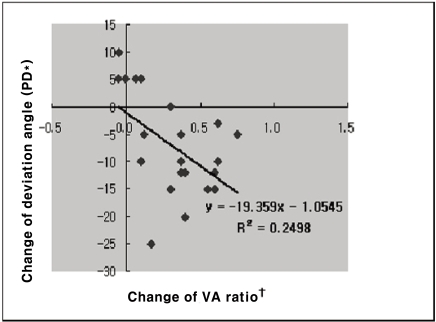
Correlation between the amount of VA ratio increase and the amount of change of deviation angle.
Spearman's correlation coefficient r=-0.479, p=0.024
PD*= prism diopter.
VA ratio†=Snellen visual acuity of the amblyopic eye/Snellen visual acuity of the sound eye.
Based on the deviation angle with glasses after occlusion therapy, patients were categorized as the surgical group with deviation within surgical limits (≥15 PD) and the non-surgical group with deviation less than 15 PD. There were considerable differences between these two groups in age at the onset of therapy (p=0.004), refractive errors (p=0.032), deviation angles with glasses before and after therapy (p=0.0001) and visual acuity ratios after therapy (p=0.003) (Table 3).

Comparison of clinical characteristics between the non-surgical group and the surgical group (Surgical limits: Deviation angle with glasses after occlusion treatment ≥ 15 PD). (Mean±SD)
Discussion
In the present study, changes in ocular alignment prior to and after occlusion therapy were evaluated in partially accommodative esotropic patients with moderate amblyopia. Our data shows that there was a significant reduction of nonaccommodative deviation angle at 2 years after occlusion therapy. Mean deviation angle with glasses was 19.45±5.97 PD at the start of occlusion therapy and decreased to 12.14± 12.96 PD at 2 years after occlusion therapy (p=0.003). Furthermore, statistical analysis revealed that there was a correlation between the increase of visual acuity of the amblyopic eye and the decrease of deviation angle (r=-0.479, p=0.024).
Results of the present study correspond with the earlier study of Koc et al.5 which reported progressive decrease of deviation angle in partially accommodative esotropia during occlusion therapy (27 PD to 11 PD). But they did not mention the depth of amblyopia and the amount of visual acuity changes during occlusion therapy. While they measured angular changes after occlusion therapy at variable periods (2~36 months, mean 12 months), we measured the amount of deviation angle at 2 years after occlusion therapy regardless of the duration of occlusion therapy. Our study focused specially on partially accommodative esotropia with moderate amblyopia.3 Furthermore, we evaluated not only the change of deviation angle but also the change of visual acuity of amblyopic eye during occlusion treatment.
These findings are in contrast to the results of Holbach et al.6 They reported that the deviation changes during occlusion treatment of strabismic amblyopic patients were not different from the fluctuation of the deviations in nonamblyopic strabismus patients after 3 months (1-13 months) of follow-up. The patients of Holbach et al.6 were nonhomogeneous esotropic group and these authors did not mention the refractive status and visual acuity changes of their patients. Kim et al.7 reported 2 cases of deterioration of accommodative esotropia during part-time occlusion. They explained that the increase of deviation angle with occlusion may simply reflect a true deviation by disruption of peripheral fusion. But the difference of visual acuities between both eyes was only one line in Snellen's chart and did not meet the diagnostic criteria of amblyopia.
The most significant finding in our study is the statistically meaningful relationship between the increase of visual acuity in amblyopic eye and the amount of decrease of deviation angle (r=-0.479, p=0.024). Mean visual acuity ratio was 0.44±0.11 at the start of occlusion treatment and increased to 0.76±0.23 at 2 years after occlusion treatment (p<0.001). These results are consistent with data, suggesting a trend to greater alignment improvement in those patients with more improvement in visual acuity.8 It seemed that as the visual acuity of the amblyopic eye increases, patients may have better fusional divergence and have a better control of their ocular alignment. It is presumed that not only the occlusion treatment but also the time spent for the treatment may be the cause of the reduction in nonaccommodative deviation angle in partially accommodative esotropic patients. Wearing glasses of full correction of refractive error during follow-up period may decrease the convergence tonus and this may have a decreasing effect of nonaccommodative deviation angle.
We were interested in unexpected differences in clinical characteristics between surgical and non-surgical groups. In the surgical group, the age at onset of strabismus was earlier and the refractive error was less hyperopic than non-surgical group. The improvement of deviation angle and visual acuity ratio were more pronounced in the non-surgical group (Table 3). Rather, we interpret our findings as evidence for partially accommodative esotropia being composed of two subtypes. The non-surgical group is postulated as decompensated accommodative esotropia with delayed treatment and the surgical group as congenital esotropia with an accommodative element being superimposed as the child grows older.
This study has important limitations, however, mostly stemming from its small sample size and retrospective design. In addition, another reason of increasing visual acuity of amblyopic eye could be the change of refractive state during occlusion treatment. Mean refractive error of amblyopic eye at the start of occlusion treatment was +2.76±2.06 D (+1.0~+7.5D) and decreased to +2.33±1.70D (+0.5~+6.5 D) at 2 years after occlusion treatment. The amount of change of refractive error is not statistically meaningful (p=0.072) but we cannot exclude the possibility that change of refractive error is another cause of increased visual acuity of amblyopic eye. This study also lacks the postoperative results of the surgical group, therefore, we are unable to correlate the occlusion treatment and postoperative ocular alignment.
The results obtained here suggest that occlusion treatment has a decreasing effect on ocular alignment in partially accommodative esotropic patients with amblyopia.
Notes
* This paper was presented in part at the 96th Annual Meeting of the Korean Ophthalmological Society, November 4th, 2006, Ilsan, Korea.