Orbital and Choroidal Plasmacytoma in Recurrent Multiple Myeloma: A Case Report
Article information
Dear Editor,
Multiple myeloma is a blood disease in which plasma cells proliferate abnormally and it accounts for approximately 1% of all cancers and 10% of hematologic malignancies [1]. Multiple myeloma is characterized by bone infiltration and it can also appear in the form of plasma cell tumors in many organs. Secondary ocular involvement is rare, but it can occur in the orbit, extraocular muscles, and within the uveal tract [2]. Intraocular plasmacytoma is very rare, but it has been reported in the iris, ciliary body, and choroid [3]. Multiple myeloma is usually treated with systemic chemotherapy and bone marrow transplantation. Focal plasmacytomas are generally treated with local radiation therapy [4,5]. We report a case of plasmacytoma that affected both the choroid and orbit in recurrent multiple myeloma.
A 56-year-old woman was diagnosed with multiple myeloma in April 2008. In October 2008, she underwent autologous peripheral hematopoietic stem cell transplantation. She received an allogeneic hematopoietic stem cell transplant in November 2013. However, multiple myeloma recurred in 2014. She was commissioned to our department for a 2-day history of orbital swelling, which was initiated during chemotherapy (2nd cycle of carfilzomib/dexamethasone after 9th cycle of lenalidomide/dexamethasone) because of recurrent multiple myeloma in June, 2018.
At the time of presentation, her visual acuity was 20 / 20 in both eyes. The intraocular pressure was 8 / 9 mmHg. There was no palpable mass, but mild swelling and a slight heating sensation were observed on the left lower eyelid. The eyeball movement was normal, and there was no proptosis. Lower orbital mass, inferior rectus muscle thickening, and choroidal mass with homogenous contrast enhancement were detected on orbital computed tomography. Wide-field fundus photography of the left eye revealed an amelanotic choroidal mass that did not involve the macula. On fluorescein angiography, the choroidal mass showed speckled hyperfluorescence. B-scan ultrasonography demonstrated a dome-shaped choroidal mass, and the A-scan peak showed high reflectivity (Fig. 1A–1D).
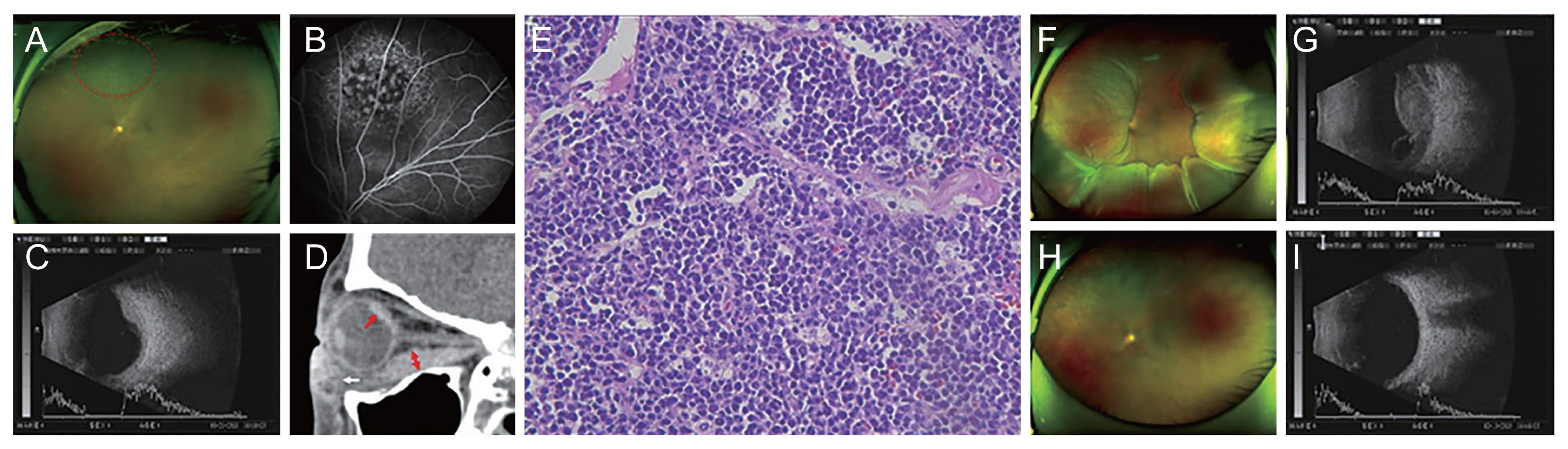
Imaging and histological examinations of plasmacytomas. (A–D) Choroidal and orbital plasmacytoma at the first presentation. (E) Histological examination of periorbital mass. (F,G) Worsening of choroidal plasmacytoma after follow up loss. (H,I) After external beam radiotherapy. (A) Wide-field fundus photography of the left eye shows round choroidal mass of mid-peripheral fundus, stippled pigmentation over the lesion (red dotted circle). (B) Fluorescein angiography of the left eye shows speckled hyperfluorescence of the lesion. (C) Ultrasonography of the left eye (B-scan mode) shows dome-shaped choroidal mass. The sclera appears normal. A-scan mode shows high reflectivity of the lesion. (D) Orbital computed tomography demonstrates homogenous enhancement of choroidal mass (red arrow) and anterior orbital mass (white arrow) and thickened inferior rectus muscle (red double headed arrows). (E) Periorbital mass with homogenous plasmacytic infiltrate (hematoxylin-eosin stain, ×400). (F) Wide-field fundus photograph of the left eye shows large choroidal mass with subretinal fluid. (G) B-scan ultrasonography demonstrates enlarged choroidal mass lesions with acoustic solidity. With A-mode, the spike amplitude within the mass shows medium-high peak. (H) Wide-field fundus photography of the left eye shows complete regression of choroidal mass. (I) No choroidal mass is found on B-scan ultrasonography after radiotherapy.
We performed tumor excision with anterior orbitotomy in the left eye, and histological examination confirmed plasmacytoma (Fig. 1E). The patient underwent systemic chemotherapy, and the choroidal plasmacytoma did not grow. As the lesion did not involve the macula, she maintained good visual acuity for 4 months.
However, the patient was subsequently lost to follow-up for nearly 4 months. When the patient returned, visual acuity of the left eye decreased to finger count 50 cm. Diffuse large choroidal mass with subretinal fluid presented as worsening of choroidal plasmacytoma (Fig. 1F, 1G). The choroidal mass did not respond to systemic chemotherapy, so the patient was managed with external beam radiotherapy (left eye [upper-lower margin 5 cm], 40, 16, 26, 40 gray), and the tumor resolved completely (Fig. 1H, 1I). However, vision of her left eye did not recover because of radiation keratitis, cataract, and retinopathy, which occurred as a complication of radiotherapy. Multiple myeloma was not responsive to chemotherapy; nevertheless, the choroidal plasmacytoma was completely resolved. The patient died 2 months later despite additional 4th cycle of pomalidomide/dexamethasone/cyclophosphamide.
Immunoglobulin G type multiple myeloma has been reported to be a risk factor for eye involvement [4]. In this case, the patient’s multiple myeloma was of immunoglobulin G kappa type. Choroidal plasmacytomas are similar to achromatic choroidal tumors, such as metastatic cancer, melanoma, nevus, and lymphoma. Therefore, fine needle aspiration biopsy is usually required to confirm the diagnosis [5]. In this case, biopsy was not performed on the choroidal mass because of the patient’s poor cooperation. The choroidal mass was not confirmed histologically as choroidal plasmacytoma, so the possibility of other amelanotic choroidal tumors other than plasmacytoma cannot be excluded. However, histological examination of the orbital mass revealed a plasmacytoma and the orbital mass was found simultaneously with choroidal mass. The choroidal mass worsened with worsening of systemic multiple myeloma, and the imaging findings showed features of choroidal plasmacytoma (Fig. 1F, 1G). According to the facts that above mentioned, it is highly possible to estimate that the choroidal mass is also plasmacytoma.
This is a very rare case of secondary ocular plasmacytoma that affected both the choroid and orbit. Secondary ocular plasmacytoma, despite its rarity, should be considered in patients with multiple myeloma when an amelanotic choroidal mass is observed. When ocular plasmacytoma occurs, it should be monitored and treated appropriately.
Notes
No potential conflict of interest relevant to this article was reported.