A Korean Woman with Reactive Lymphoid Hyperplasia of the Uvea
Article information
Dear Editor,
Recently, we diagnosed a 50-year-old woman as having reactive lymphoid hyperplasia (RLH) of the uvea, and herein we report that this is the first diagnosis of this condition in a Korean patient. The patient was referred to the ophthalmology clinic with blurry vision due to choroidal mass-like lesions of the right eye for 1 month. Uncorrected visual acuity (UCVA) of the right eye was 0.2, and best-corrected visual acuity of the right eye was 0.9 (+sph 2.25, -cyl 0.75, axis 90). Slit lamp examination showed no remarkable findings in the anterior segment including the vitreous. Fundus examination via indirect ophthalmoscopy showed multiple yellow-orange colored choroidal mass-like lesions at the posterior pole in the right eye (Fig. 1A). Fluorescence angiography showed stippled hyperfluorescence (Fig. 1B) with late phase staining (Fig. 1C). On indocyanine green angiography, retinochoroidal folds radiating from the optic nerve head were seen as hypofluorescence lines upon examination (Fig. 1D and 1E). Spectral domain optical coherence tomography showed subretinal fluid in the fovea, with undulating retina due to choroidal mass both horizontally (Fig. 1F) and vertically (Fig. 1G). Ultrasound sonography showed homogenous intraocular elevation which was acoustically empty (Fig. 1H), and lesion size was base 11.93 mm with a height of 2.71 mm. On magnetic resonance imaging of the brain and orbit, the subretinal mass showed hyperintensity on T1 (Fig. 1I) and hypointensity on T2 images (Fig. 1J). Systemic evaluation including positron emission tomography revealed no primary malignancy, and ocular management was recommended by the oncologist. RLH of the uvea was suspected, and systemic steroid treatment was started with prednisolone 50 mg per day for the first week, and then 40 mg per day for the following week. After 2 weeks, UCVA of the right eye improved to 0.8, and choroidal elevation was also improved (Fig. 1K). On ultrasonography, the size of the choroidal mass was base 8.80 mm with a height of 1.87 mm (Fig. 1L). Systemic steroid administration was continued at 30 mg per day for one week, followed by 25 mg per day for an additional week. UCVA of the right eye after one month of steroid treatment was 0.6, and the choroidal mass lesion was stable, and steroid administration was further tapered off.
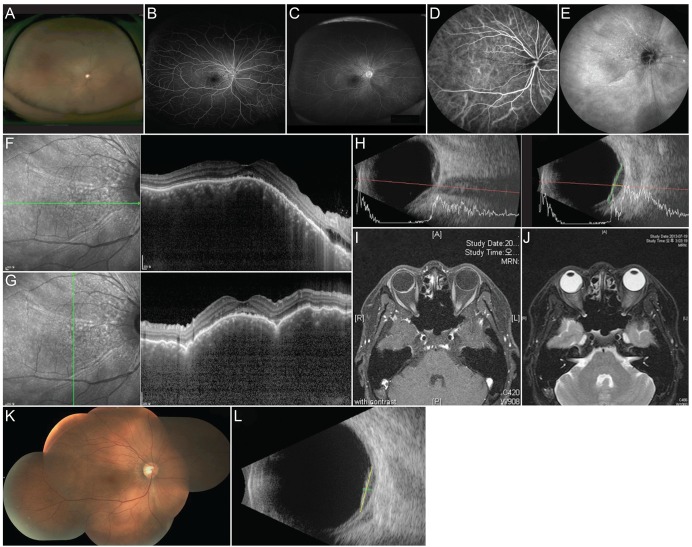
Fundus photography of the 50-year-old patient with reactive lymphoid hyperplasia of the uvea in the right eye (A). Fluorescence angiography showed stippled hyperfluorescence (B) with late phase staining (C). On indocyanine green angiography, retinochoroidal folds radiating from the optic nerve head were seen as hypofluorescence lines throughout examination (D,E). Spectral domain optical coherence tomography showed subretinal fluid at fovea, with undulating retina due to choroidal mass both horizontally (F) and vertically (G). Ultrasound sonography showed homogenous intraocular elevation which was acoustically empty (H), and lesion size was base 11.93 mm with height 2.71 mm. On magnetic resonance imaging of brain and orbit, the subretinal mass showed hyperintensity in T1 (I), and hypointesnity on T2 images (J). After systemic treatment with steroid for 2 weeks, choroidal elevation was improved (K). On ultrasonography, size of choroidal mass was measured as base 8.80 mm with height 1.87 mm (L).
RLH of the uvea is a rare disease, and it is a diagnosis of exclusion. RLH usually affects middle-aged patients, with a mean age of 55 years [1]. RLH is generally unilateral, and has no apparent racial or sexual predilection [2]. Patients suffer from recurrent episodes of blurred vision and metamorphopsia secondary to serous fluid serous detachment of the macula [1,2,3,4,5]. Multifocal yellow-orange lesions by choroidal infiltration are a typical feature of RLH of the uvea, and sometimes pink, smooth-surfaced subconjunctival extensions are reported [1,2,3,4,5]. Ultrasonographic findings are especially helpful in the diagnosis of RLH in that they reveal diffuse choroidal infiltration with low internal reflectivity, a lack of choroidal/scleral excavation, and the presence of extrascleral peripapillary nodules [4,5]. RLH usually responds to steroid therapy promptly [4,5]. Before the diagnosis of RLH, several diseases should be considered including diffuse choroidal melanoma, metastatic carcinoma, inflammatory diseases such as multifocal choroiditis, uveal effusion, and malignant lymphoma [3]. Although it is rare, we experienced a Korean patient who was compatible with RLH, and this patient was successfully treated with systemic steroid treatment. Therefore, when diagnosing choroidal mass in the Korean population, RLH should be also considered.
Notes
No potential conflict of interest relevant to this article was reported.