Changes in Spherical Aberration after Various Corneal Surface Ablation Techniques
Article information
Abstract
Purpose
The corneal change induced by refractive procedures influence both the postoperative refractive status and the ocular spherical aberration (SA). We evaluated changes in corneal SA after three types of surface ablation: phototherapeutic keratectomy (PTK), myopic photorefractive keratectomy (PRK), and myopic wavefront-guided laser epithelial keratomileusis (LASEK).
Methods
Twenty-six eyes (25 patients) were subjected to PTK 26 eyes (14 patients) to PRK, and 34 eyes (17 patients) to wavefront-guided LASEK. Corneal SA was measured with the iTrace in all patients both preoperatively and 6 months postoperatively.
Results
Six months after surgery, mean corneal SA was -0.173 ± 0.171 µm in the PTK group, 0.672 ± 0.200 µm in the PRK group, and 0.143 ± 0.136 µm in the wavefront-guided LASEK group. The mean difference between the preoperative and postoperative corneal SA (ΔSA) was -0.475 µm in the PTK group, 0.402 µm in the PRK group, and -0.143 µm in the wavefront-guided LASEK group.
Conclusions
Surgically induced changes in corneal SA vary with procedure. The prediction of the pattern of SA change induced by various surface ablation procedures may be helpful for developing future surgical procedures.
Surface ablation using an excimer laser was introduced as a mode of refractive surgery about two decades ago. The main concerns in the early period of the surgery were attaining good outcomes such as improved visual acuity, correction of refractive errors, better night vision, and enhanced contrast sensitivity. Considering the age of patients who undergo refractive surgery [1], the patient's status after surgery has assumed increased importance. Spherical aberration (SA) is an important factor which can influence vision quality in older individuals [2]. Though the variation in the corneal SA of unoperated eyes is relatively small and usually falls within an expected range, lens-induced SA rises with age [3]. However, refractive procedures also inevitably alter corneal SA and the extent of the change varies by procedure. Some reports have found that laser in situ keratomileusis (LASIK) and photorefractive keratectomy (PRK) procedures tended to increase postoperative corneal SA, but to varying extents [4-7]. After myopic correction, corneal SA changed to a more positive value [7], while after hyperopic correction, corneal SA changed from a positive to a negative value [8]. It is obvious that phototherapeutic keratectomy (PTK) will affect the postoperative corneal SA, though precisely how it does this has not yet been elucidated. Such changes in corneal SA are especially important when patients undergo surface ablation prior to cataract surgery. Recent designs of aspheric intraocular cataract lens (IOLs) are based on the concept of aberration modification, whereby a patient's functional vision is improved by compensating for a positive corneal SA [9]. We performed the current study to compare and predict the patterns of postoperative changes in SA after three kinds of surface ablation: PTK, PRK, and wavefront-guided laser epithelial keratomileusis (LASEK).
Materials and Methods
Ninety-six eyes (56 patients) were subjected to corneal surface ablation and were included in the present study. Twenty six eyes (25 patients) were treated with PTK, 26 eyes (14 patients) with conventional PRK, and 34 eyes (17 patients) with wavefront-guided LASEK. All patients received preoperative ophthalmic examinations including slit lamp microscopy, fundus examination, cycloplegic and manifest refraction assessment, corneal pachymetry, and topography measurements. Patients with diabetes, connective tissue disease, glaucoma, or retinal disease were excluded.
All surface ablation procedures were performed using a VISX STAR S4 excimer laser platform (Abbott Medical Optics, Santa Ana, CA, USA); each procedure within any particular type was performed using the same protocol. Wavefront analysis using Wavescan (Abbott Medical Optics) was used in wavefront-guided LASEK procedures. The treatment zone diameter was 8.0 mm for PTK, and 6.0 to 6.5 mm for PRK and LASEK. The ablation depth of PTK ranged from 50 to 152 mm depending on patient condition.
The PTK procedure was performed with a radiant exposure of 160 mJ/cm2. After insertion of a lid speculum, the epithelium was removed mechanically with a spatula. An ablation zone of 6.0 mm with no transition zone at a pulse rate of 10 Hz was used for all eyes. The density and depth of the remaining diffuse stromal haze were checked after each 5 to 10 µm excimer laser ablation to prevent over-ablation. Preservative-free hydroxypropyl methyl cellulose eye drops (Tears Naturale Free; Alcon Laboratories, Fort Worth, TX, USA) were instilled during the procedure every 10 µm to ensure the smoothness of the ablation, and the depth of the ablation was recorded. For conventional PRK, a 7.0-mm optical zone marker was applied to the cornea. A crescent knife was then used to remove the central 7.0 mm of the corneal epithelium. The loose epithelium was removed using a blunt spatula and followed by stromal ablation using the conventional mode for refractive errors correction.
Wavefront-guided excimer laser ablation was performed using the STAR S4 IR laser system (Abbott Medical Optics) with iris registration. A speculum was applied to the eye and 20% alcohol was applied for 30 seconds and then carefully washed off with balanced salt solution. The epithelium was detached as a single sheet toward the 12-o'clock position using a spatula. The epithelium was carefully repositioned with a spatula.
Corneal SA (the Z04 parameter of the Zernike coefficients) was measured in pupils dilated more than 6-mm pupil with myadriatics (Mydrin-p; Santen, Osaka, Japan) preoperatively and 6 months postoperatively in all patients using an iTrace (Tracey Technologies, Houston, TX, USA). SA was rescaled for pupil diameters of 4 mm using iTrace.
iTrace evaluates entire ocular or separate corneal and internal optics with their own analyzing processes and displays each of them simultaneously in one screen. In the statistical analysis, paired t-tests were employed to compare the preoperative and postoperative SA in each surface-ablation group and the mean differences in SA were identified.
Results
The clinical and demographic characteristics of the patients are summarized in Table 1. PTK was employed for the reduction of corneal opacity caused by granular type 2 corneal dystrophy. The preoperative SA levels in the three groups were compared and showed no clinical difference (p = 0.053). Refractive procedures (PRK and LASEK) were performed for the correction of myopic and/or astigmatic refractive errors. Six months after each procedure, the corneal SA was measured. The mean corneal SA changed from 0.291 ± 0.094 mm (preoperative) to -0.177 ± 0.158 (postoperative) in patients treated with PTK. The mean postoperative corneal SA was 0.672 ± 0.200 in patients who underwent PRK and 0.092 ± 0.117 mm in patients treated with wavefront-guided LASEK. In all groups, the mean postoperative corneal SA differed significantly from the mean preoperative value. The differences between preoperative and postoperative SAs (ΔSA values) are shown in Table 2 and Fig. 1. The mean ΔSA was -0.468 ± 0.123 mm (range, -0.655 to -0.258 mm) in the PTK group, 0.402 ± 0.197 mm (range, 0.057 to 0.881 mm) in the PRK group, and -0.194 ± 0.135 mm (range, -0.409 to 0.061 mm) in the wavefront-guided LASEK group. The distribution of ΔSA was distinct for each group.

Demographic and clinical characteristics of our patients

Changes in corneal SA with surgery, according to surface ablation procedure
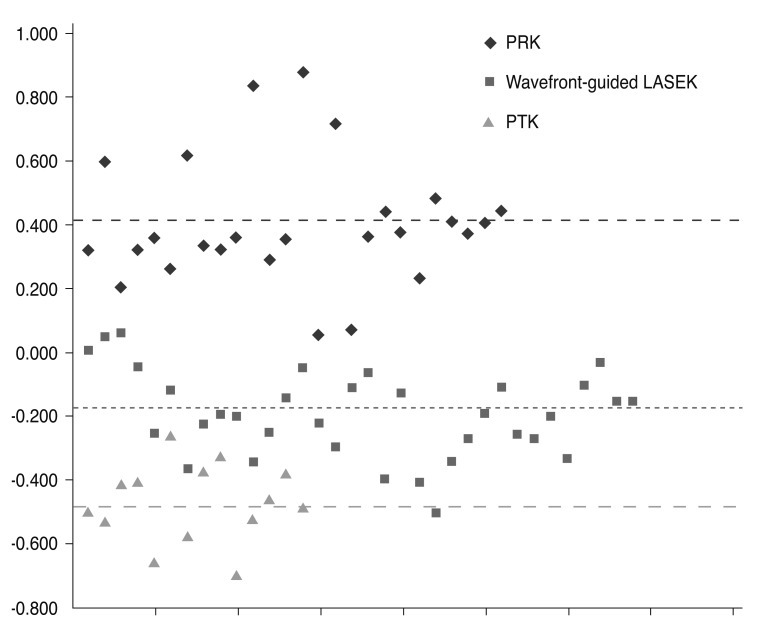
Distribution of differences between preoperative and postoperative spherical aberration (SA) values (ΔSA). The mean ΔSA of each group is indicated with dotted lines. PRK = photorefractive keratectomy; LASEK = laser epithelial keratomileusis; PTK = phototherapeutic keratectomy.
Discussion
Myopic correction procedures, including PRK, LASIK, and LASEK, are known to increase positive SA and higher-order aberrations [4-7]. Because surface ablation procedures for refractive corrections result in oblate corneal centers, the cornea loses natural negative asphericity [5]. In the current study, the maximum increase in mean corneal SA was observed in the conventional PRK group (ΔSA = 0.402 mm, p < 0.0001). The mean corneal SA value in the wavefront-guided LASEK group decreased (ΔSA = -0.194 mm, p < 0.01), which almost eliminated ocular SA. Some reports on the value of wavefront-guided ablation profiles for customized ocular aberrations have appeared, but the results have been contradictory. Winkler von Mohrenfels et al. [10] reported that wavefront-guided LASEK reduced corneal SA, whereas Chung et al. [11] claimed that the procedure slightly increased corneal SA. However, even in studies showing increased postoperative SA, the amount of wavefront-guided LASEK-induced increases was significantly smaller than that seen after conventional procedures [11,12]. In the current study, wavefront-guided LASEK was associated with decreases in surgically induced corneal SA and ocular SA. To the best of our knowledge, this is the first study to evaluate changes in corneal SA after PTK. Considering the possible diversity in corneal status in the PTK group, we initially confirmed that there was no difference in mean preoperative corneal SA level between the three groups. Previous work has revealed a rise in positive SA after myopic correction, and an induction of negative SA when hyperopic correction was performed [13-16]. In contrast to other refractive procedures, PTK uniformly ablates the treatment zone and was expected to have only a small effect on asphericity or to result in a mixed pattern of myopic and hyperopic ablation. A previous report showed that the relatively lower energy delivered at the peripheral ablation zone during PTK resulted in a hyperopic shift [17]. Based on this, PTK may induce a positive SA because of the oblate central area. However, our results suggest that the cornea became more prolate after PTK, indicating that the procedure induced a negative SA. For an explanation of this effect, we evaluated the typical corneal aberration image of each procedure (Fig. 2). This figure showed a small central island at the corneal center in a PTK eye. The images showed a small flattening at the cornea center in PRK eyes and a relatively large flattened corneal center in wavefront-guided LASEK eyes. Because the PTK procedure using the VISX STAR S4 excimer laser platform ablated the cornea based on a broad beam profile, an apparent central corneal island was observed in most of the PTK cornea. Therefore, the central elevation of the cornea may be related with the negative shift of SA after the PTK procedure. The mean difference in corneal SA after PTK was -0.468 mm (p = 0.006).
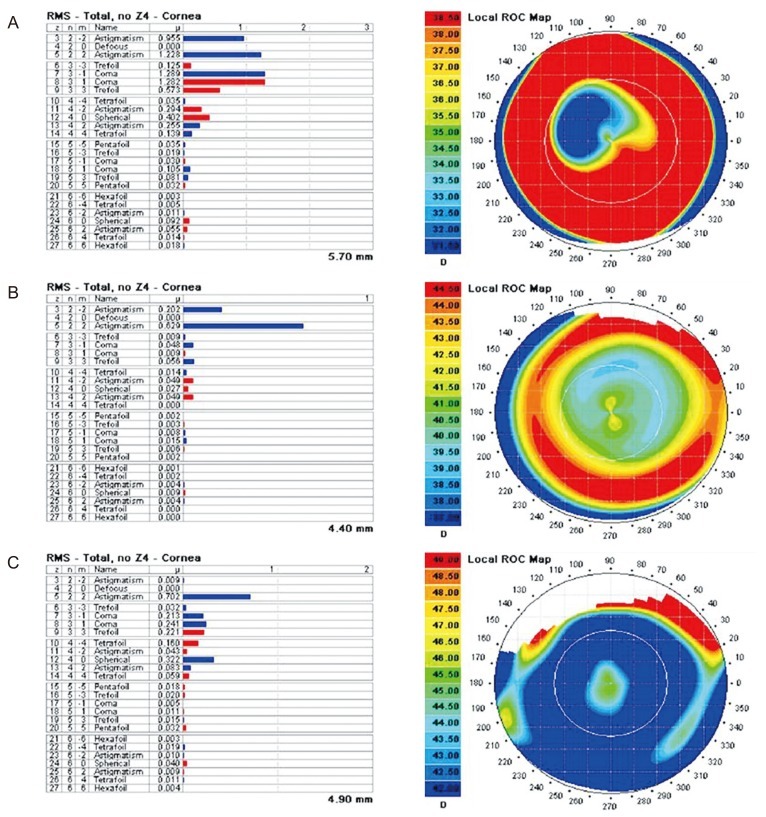
Output of the iTrace aberrometer showing Zernike coefficients for the corneal wavefronts of patients who underwent three different kinds of surface ablation procedures. (A) A photorefractive keratectomy patient. In this example, Z04 = +0.402 µm, indicating increased corneal spherical aberration. (B) A laser epithelial keratomileusis patient. In this example, Z04 = 0.027 µm, indicating a small amount of corneal spherical aberration; (C) A phototherapeutic keratectomy patient. In this example, Z04 = -0.322 µm, indicating negative spherical aberration. RMS = root mean square; ROC = radius of curvature.
Each surface ablation procedure showed a typical pattern of postoperative changes in SA, which can also be applied to aberrational modification during the planning of cataract surgery. Another important consideration for aberration modification is the optimal SA target. Although the general concept behind wavefront-guided ablation is reducing corneal SA, the complete elimination of SA may not be the best manner in which to obtain the best functional vision. Recent studies indicate that a maximum reduction of postoperative SA does not correlate with the best contrast sensitivity, depth of field, or subjective visual quality [18-21]. Some studies have achieved good results with a target of zero ocular SA [22,23]. However, another report demonstrated better contrast sensitivity with use of an aspheric IOL [24] designed to achieve a target ocular SA of 0.10 mm on the basis of earlier studies on supernormal vision (visual acuity 20 / 15 or better) [25]. Other research suggests that ocular SA increases the depth of focus, and that the elimination of SA could reduce the tolerance to defocus [21]. Koch and Wang [26] found that optimal visual performance was determined not only by ocular SA but also by defocus and interaction with all higher-order aberrations. Despite this controversy over the optimal target of SA, with further studies needed, the current project is based on the principle that the reduction of excessive corneal SA will lead to better functional vision.
In the present study, the postoperative corneal SA was different in each surface ablation group and showed a distinct pattern for each procedure. PTK is a therapeutic option and not a pure refractive procedure. The major goal of the procedure is the removal of corneal tissue to eliminate opacity, not any SA changes induced by the procedure. In addition, there is to date no program specifically designed to modify SA. In this study, we could predict the pattern of ocular aberration changes after PTK procedures.
Acknowledgements
This work was partially supported by the Converging Research Center Program funded by the Ministry of Education, Science and Technology (2011K000680).
Notes
No potential conflict of interest relevant to this article was reported.