Posterior Subtenon Triamcinolone Acetonide in Gas-filled Eyes as an Adjunctive Treatment for Complicated Proliferative Diabetic Retinopathy
Article information
Abstract
Purpose
To evaluate the effect of adjunctive subtenon injection of triamcinolone acetonide (TA) in gas-filled eyes after vitrectomy for complicated proliferative diabetic retinopathy (PDR).
Methods
This nonrandomized comparative study included 27 patients (27 eyes) who underwent pars plana vitrectomy and gas tamponade for treatment of PDR with tractional or combined tractional-rhegmatogenous retinal detachment and who received subtenon injection of TA (40 mg) at the end of surgery. The study group was compared with the control group (29 eyes), which was matched with the study group for preoperative and intraoperative parameters, but underwent pars plana vitrectomy and gas tamponade without a subtenon injection of TA.
Results
Retinal reattachments without reoperation were achieved in 25 eyes (92.6%) and 26 eyes (89.7%) at 6 months (p = 1.000) in the study and control groups, respectively. The study group and the control group did not differ significantly in the frequency of postoperative proliferative vitreoretinopathy, retinal redetachment rate, reoperation rate, macular pucker formation, postoperative vitreous hemorrhage, gain in visual acuity, intraocular pressure, and intraocular inflammation (p > 0.05).
Conclusions
The clinical results of pars plana vitrectomy for complicated PDR are not improved significantly by an adjunctive subtenon TA injection in gas-filled eyes.
Triamcinolone acetonide (TA) is a long-acting and relatively insoluble corticosteroid with reported efficacy when injected by intravitreal or subtenon methods as an adjunctive treatment for inflammatory, proliferative, neovascular, or edematous eye diseases [1-8].
Since TA has been shown to suppress unwanted intraocular proliferation of cells, reduce inflammation, stabilize the blood-ocular barrier, and downregulate the production of vascular endothelial growth factor [9-13], TA was thought to be a potentially useful additional tool in the treatment of proliferative diabetic retinopathy (PDR). Actually, some studies have demonstrated that intravitreal TA injection as an adjunctive procedure in pars plana vitrectomy for PDR reduces postoperative intraocular inflammation and is effective in the prevention of recurrent vitreous hemorrhage [7,14].
Intraocular gases in vitreoretinal surgery are widely used. In conjunction with advanced surgical techniques, intraocular gases have improved the ability to successfully treat retinal detachments that have been made more complicated by proliferative vitreoretinopathy (PVR), giant tears, and posterior tears.
Thompson et al. [15] used sulfur hexafluoride (SF6) for tamponade of suspected retinal breaks or to prevent postoperative vitreous hemorrhage. Yang et al. [16] evaluated the hemostatic effect of intravitreal injection of perfluoropropane (C3F8, 10%) and concluded that it may reduce the rate of recurrent vitreous hemorrhage. Farrahi et al. [17] also revealed that SF6 (20%) in the vitreous cavity provides temporary tamponade and reduces the incidence of postoperative diabetic vitreous hemorrhage.
However, on review of the literature, no clinical studies were found on the use of posterior subtenon TA in gas-filled eyes with PDR. When localized steroid therapy is needed to reduce postoperative intraocular inflammation, intravitreal triamcinolone acetonide (IVTA) has been shown to be effective. IVTA is more invasive and also has a risk for intraocular pressure (IOP) elevation. Therefore, we thought that a posterior subtenon triamcinolone injection of TA could be used safely to lower the inflammatory reaction with less risk of IOP elevation. We wanted to obtain both a faster recovery time and maintain a normal IOP after vitrectomy. Therefore, we investigated the clinical outcome of patients who received a subtenon TA injection in gas-filled eyes after vitreoretinal surgery for complicated PDR.
Materials and Methods
Twenty-seven eyes of 27 patients who underwent pars plana vitrectomy for treatment of PDR with tractional or combined tractional-rhegmatogenous retinal detachment, with/without vitreous hemorrhage, were included in this study. Exclusion criteria were patients with previous ocular surgery, history of any ocular disease or trauma, intravitreal silicone oil injection during surgery, previous intravitreal bevacizumab or TA injection, and previous posterior subtenon injection of TA. Patients who did not receive gas injection during surgery were also excluded. If there was a failure to execute the injection properly, the triamcinolone acetonide was regurged, and the case was excluded. Informed consent was obtained from all patients after a full explanation of the potential effects of a subtenon TA injection.
Surgery was carried out under general or retrobulbar anesthesia. The standardized technique of pars plana vitrectomy was performed using three 20-gauze pars plana sclerotomies. The vitreous was removed up to the vitreous base and the posterior vitreous surface. Phakic eyes underwent lens extraction and IOL implantation. Depending on the clinical situation, additional procedures were performed, such as peeling, delamination, and segmentation of membranes, temporary application of perfluorocarbon liquids, and relaxing retinotomies. Then, panretinal endolaser photocoagulation including periphery was performed. Before closing the sclerotomy sites, C3F8 (15%) was used as a tamponade in all eyes. After closing the sclerotomy sites at the end of the operation, 40 mg of TA was injected into 27 eyes in the study group. The TA was slowly injected through the conjunctiva and tenon's capsule and applied to the bare sclera near the superotemoral fornix using a curved cannula. After the application was complete, gentle pressure was maintained by a sterile swab along the path of the cannula to avoid TA reflux. All the patients were operated on by the same retinal surgeon (YHP). All patients were examined by the operator during the 6 months follow-up period. At each visit, best-corrected visual acuity, IOP, intraocular inflammation, retinal redetachment rate, PVR, postoperative vitreous hemorrhage, macular pucker formation, and the need for further vitreoretinal reoperation were measured. Snellen visual acuities measured at each visit were converted to the logarithm of the minimum angle of resolution (logMAR) scale for statistical analysis. Intraocular inflammation in the anterior chamber was graded on a scale of 0 to 4; where 0 = none, 1 = mild, 2 = moderate, 3 = severe, and 4 = very severe. The extent of vitreous re-bleeding was graded according to the following scales: 0 = no vitreous hemorrhage, 1 = mild vitreous hemorrhage with visible fundus details, 2 = moderate vitreous hemorrhage with no visible fundus details but with an orange fundus reflex, 3 = severe vitreous hemorrhage with no fundus details and no fundus reflex. PVR was graded according to four grades (A, B, C, and D), suggested by Retina Society Terminology Committee [18].
The study group was compared with a control group consisting of 29 eyes (29 patients) with complicated PDR with tractional or combined tractonal-rhegmatogenous retinal detachment, with/without vitreous hemorrhage. The patients of the control group, which was formed retrospectively, were matched with those of the study group for age, sex, duration and type of diabetes, prevalence of hypertension, lens status, previous treatment of laser photocoagulation, preoperative refractive error, and preoperative IOP (Table 1). Patients in the control group also underwent pars plana vitrectomy and C3F8 gas temponade in a similar way as the patients in the study group. The operations were performed by the same surgeon who used the same technique and instruments. However, the patients in the control group did not receive a subtenon injection of TA at the end of the surgery.
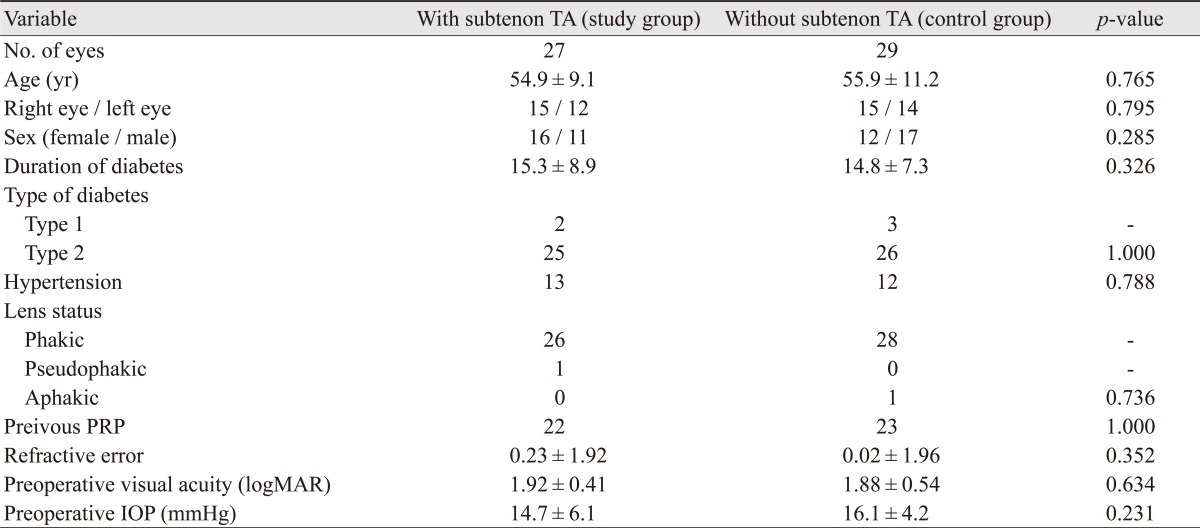
Demographics and clinical characteristics of patients who underwent vitrectomy and gas tamponade with/without subtenon injection of TA for complicated proliferative diabetic retinopathy
Results
Clinical characteristics and demographics of the both groups are described in Table 1. Follow-up period in the both groups was 6 months. The two groups were comparable in terms of demographics and preoperative factors (Table 1). Single-operation retinal reattachment was achieved in 25 eyes (92.6%) 6 months after surgery in the study group and in 26 eyes (89.7%) in the control group. Retinal redetachment occurred in 2 eyes (7.4%) in the study group and in 3 eyes (10.3%) in the control group over the course of 6 months. The differences between the two groups were not significant (p = 1.000). Postoperative PVR developed in 4 eyes (14.8%) (3 eyes with grade B, and 1 eye with grade C) in the study group and 7 eyes (24.1%) (4 eyes with grade B, and 3 eyes with grade C) in the control group. There was no statistically significant difference in PVR development between the two groups (p = 0.506). Macular pucker developed in 1 eye (3.7%) in the study group and 3 eyes (10.3%) in the control group. Two eyes (7.4%) in the study group required reoperation for retinal redetachments, and 4 eyes (13.8%) in the control group required reoperation for retinal redetachments (3 eyes). In the control group, one eye developed a significant macular pucker. The frequencies of reoperation and macular pucker formation did not differ significantly between the two groups (p = 0.671, p = 0.612). Although the differences in postoperative PVR development, reoperation, and macular pucker formation between two groups were not statistically significant, the frequencies of those were lower in the study group than in the control group.
LogMAR visual acuity determined at 6 months after the operation was 0.49 ± 0.47 in the study group and 0.54 ± 0.42 in the control group. There was no significant difference between the two groups (p = 0.154). Significant improvement in visual acuity was observed in both groups. However, the differences between the two groups were not significant (p = 0.793). The mean improvement of visual acuity was 1.43 ± 0.73 logMAR units in the study group and 1.34 ± 0.69 logMAR units in the control group (Table 2). There was no statistically significant difference in IOP between the two groups at any point of the follow-up period (p > 0.05) (Table 2). Two eyes in the study group and two eyes in the control group had a temporary IOP rise in excess of 21 mmHg. In the both groups, there were no significant difference in intraocular inflammation since the first postoperative day (p > 0.05) (Table 2). Vitreous hemorrhage after the pars plana vitrectomy occurred in 2 eyes (7.4%, 2 eyes in grade 1) in the study group and in 3 eyes (10.3%, 3 eyes in grade 1) in the control group. There was no significant difference in the rate of postoperative vitreous hemorrhage between the two groups (p = 1.000). Iris neovascularization was absent in the study group, but developed in 1 eye (3.4%) in the control group during the 6 months follow-up period. There was no significant difference in the rate of iris neovascularization between the two groups (p = 1.000). No cases of endophthalmitis or neovascular glaucoma occurred postoperatively in both groups.
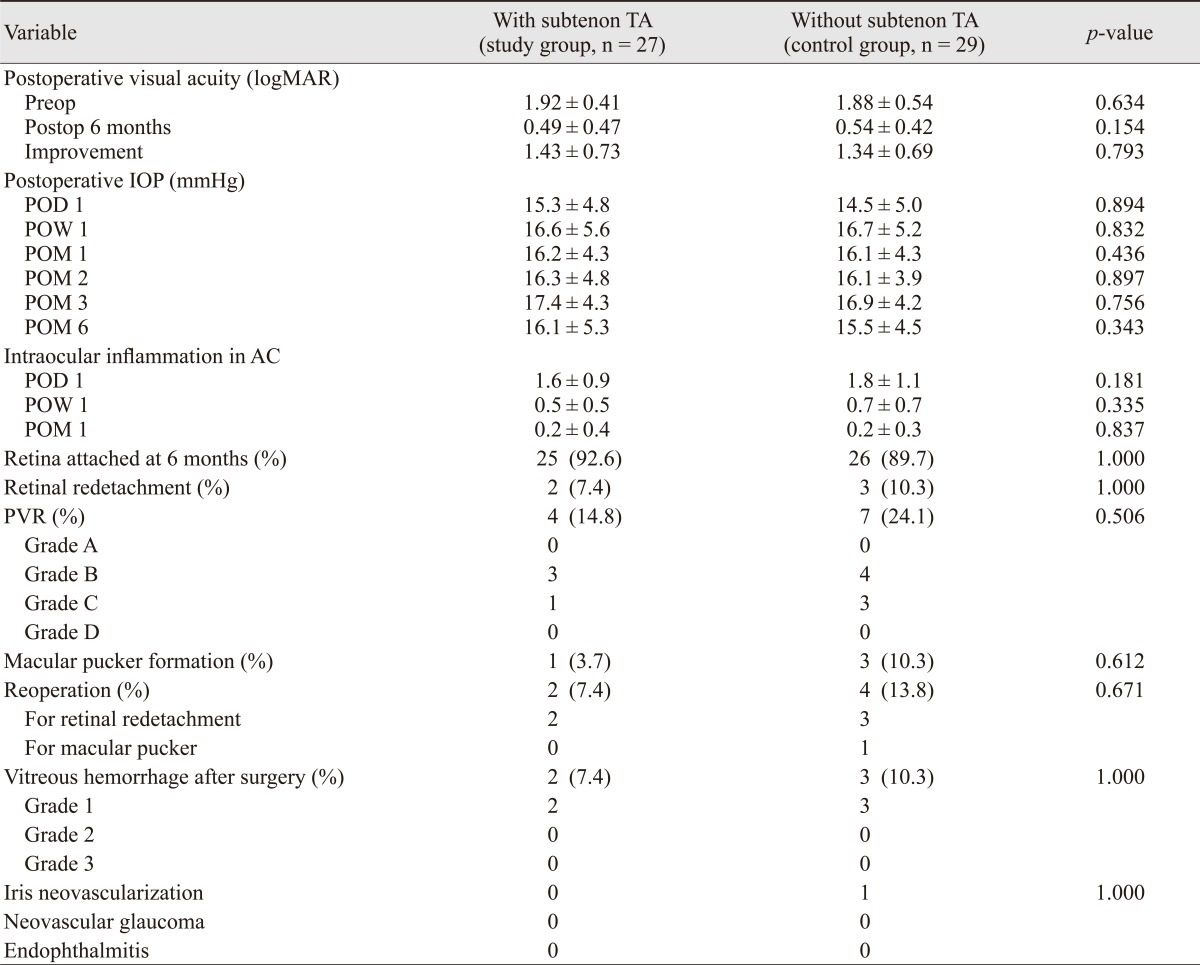
Postoperative data for the study group undergoing vitrectomy and gas tamponade with subtenon injection of TA at the end of the surgery and the control group undergoing vitrectomy and gas tamponade without subtenon injection of TA
Discussion
The effect of subtenon TA as an adjunctive treatment in gas-filled eyes in patients with complicated PDR was evaluated in this non-randomized comparative study. Although TA has been used as an intravitreal adjunctive treatment for PDR and retinal detachment with PVR [7,19-21], and as posterior subtenon injection for visual loss caused by retinal edema and other reversible inflammatory diseases [22,23], there have been no studies to our knowledge to investigate the clinical results of a subtenon TA injection in gas-filled eyes. Regarding intravitreal TA as an adjunctive treatment for PDR, there were conflicting results. Faghihi et al. [14] reported patients with intravitreal TA injection at the end of vitrectomy had better visual acuity outcomes, lower re-bleeding, and reoperation rates compared with other patients that didn't receive intravitreal TA. Conversely, Jonas et al. [24] reported intravitreal TA appeared not to be helpful when used as an adjunctive treatment.
In the present study, the eyes of the study group receiving the subtenon TA injection and the eyes of the control group without the subtenon TA injection did not differ significantly in the rate of postoperative PVR development, retinal redetachments, macular pucker formation, reoperation, and postoperative vitreous hemorrhage. In agreement with these findings, the mean improvement of visual acuity through the entire follow-up period and the visual acuities at the end of the study did not differ between the two groups. Regarding the present study, one may infer that the subtenon TA used as an adjunct in gas-filled eyes did not have a significant anti-proliferative property and did not improve the final visual results.
Steroids injected into the globe stabilize the blood-retinal barrier and inhibit the secretion of vascular endothelial growth factor, which could decrease the vascular permeability and result in the prevention of macular edema and increase of visual acuity [4,25-30]. It may also inhibit the stimulation and migration of retinal endothelial cells, reduce the rate of fibrous proliferation and tractional retinal detachment, and suppress the angiogenesis by decreasing many inflammatory cytokines secretions [30-32]. All of these effects could help to reduce the various complications related to proliferative diabetic retinopathy and to decrease the reoperation rate. However, our clinical results in gas-filled eyes indicated that subtenon TA injection did not seem to have any beneficial effects in anti-proliferative outcomes and visual acuity. The results in this study may be caused by several reasons. First, TA itself as an adjunctive treatment is not associated with better clinical outcomes. Secondly, a single injection of TA is not enough to produce better clinical results. Lastly, the adjunctive effects of TA through the trans-scleral route are not significant. As far as we know, several studies have shown that a subtenon injection of TA is effective for treating chorioretinal inflammatory diseases [23,33].
Shen et al. [34] have studied the pharmacokinetics of triamcinolone acetonide after a single 40 mg posterior subtenon application. In their study, a posterior subtenon TA injection can provide a high local TA level (8,632 ng/day/mL for aqueous, 1,262 ng/day/mL for vitreous) in ocular tissues but yields a low level of TA in systemic circulation (17.4 ng/day/mL for plasma). TA entered the aqueous more rapidly than it entered the vitreous, which had an obvious absorption phase during the first 24 hours.
In either case, the injection of subtenon TA did not seem to be helpful when used as an adjunctive tool in a gas-filled eye. Although the study population and its design were different from the present study, Entezari et al. [35] insisted that the subtenon route failed to show a significant effect because of inadequate penetration through sclera, mentioning posterior subtenon TA injection had no therapeutic effects on refractory diabetic macular edema.
One of the major concerns after intravitreal TA injection is an increased IOP. An elevation of IOP has been reported in many eyes undergoing intravitreal injection of TA for management of various ocular diseases [36-40]. However, the elevation of IOP is not a major problem in eyes receiving a subtenon injection of TA [41]. This agrees with our study in which the number of eyes experiencing IOP elevation in excess of 21 mmHg was just two in each group, and the pressure rise in the two eyes in the study group returned to a normotensive level on subsequent examination without any antiglaucomatous therapy. However, it was not certain whether the IOP elevation was caused by the subtenon TA injection.
Although this study provided for consistent surgical technique from one retinal surgeon and the same instruments to reduce the influence of external factors, there were certain limitations. First, the number of patients and the follow-up period were limited. A larger number of eyes might have proved the beneficial effect of subtenon TA in gas-filled eyes, and a longer period of follow-up may have resulted in different clinical results to some extent. Secondly, the extremes of disease severity were not stratified. Finally, the study was not a randomized prospective investigation.
In conclusion, the results of the present study suggest that the outcomes of vitrectomy in complicated proliferative diabetic retinopathy have not been improved by subtenon TA injection in gas-filled eyes. Despite the theoretical advantages of the anti-inflammatory and anti-angiogenic effects of TA, TA used as a subtenon adjunct in gas-filled eye is not strongly suggested for the treatment of complicated PDR until more large scale studies prove a therapeutic benefit of TA. In the future, we are planning to compare the effect of a TA injection in a randomized circumference to make sure of TA's effectiveness.
Notes
No potential conflict of interest relevant to this article was reported.