

An overhanging bleb is a complication of glaucoma filtration surgery. Intervention is useful to cure the induced foreign body sensation, epiphora, astigmatism, and associated decrease in visual acuity. Various treatment modalities, including cryotherapy, laser, and surgical excision, have been described; however, these may cause damage to the thin cystic walls of the blebs, which underwent prior anti-metabolite therapy, leading to leakage and hypotony. Here, we report safe excision of the overhanging portion of a large, multi-loculated, cystic bleb following autologous blood injection and compression suture placement.
Case Report
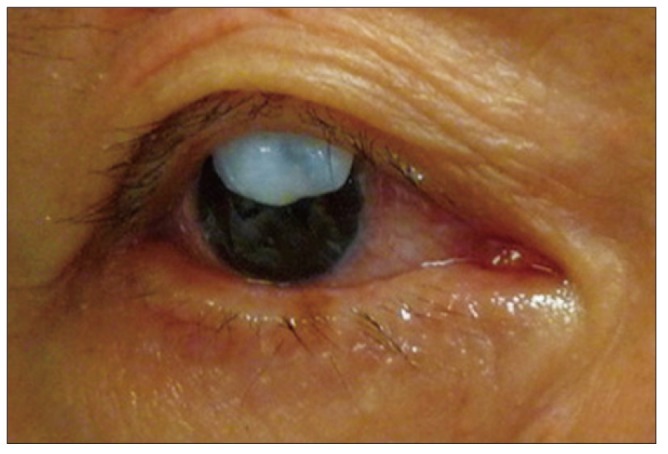
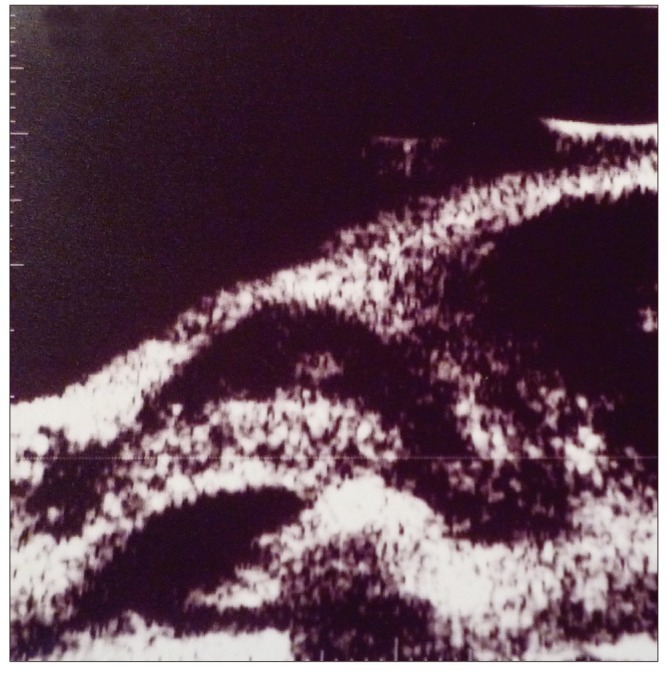
A 64-year-old man with history of chronic angle closure glaucoma underwent right eye trabeculectomy with mitomycin C 4 years prior, followed by phacoemulsification with intraocular lens implant 2 years prior, presented with a 6-month history of a foreign body sensation, epiphora, and blurring. Previous right eye best corrected visual acuity was 20 / 30 after cataract surgery and was reduced to 20 / 80 at presentation. Goldman applanation intraocular pressure (IOP) was 8 mmHg. Slit-lamp examination revealed a large, superior overhanging cystic bleb encroaching onto the corneal surface (Fig. 1). Ultrasound biomicroscopy revealed multiple loculations within the bleb (Fig. 2). The septa between the loculated compartments within the bleb appeared thin and a high risk of injury was anticipated with simple partial excision of the overhanging portion.
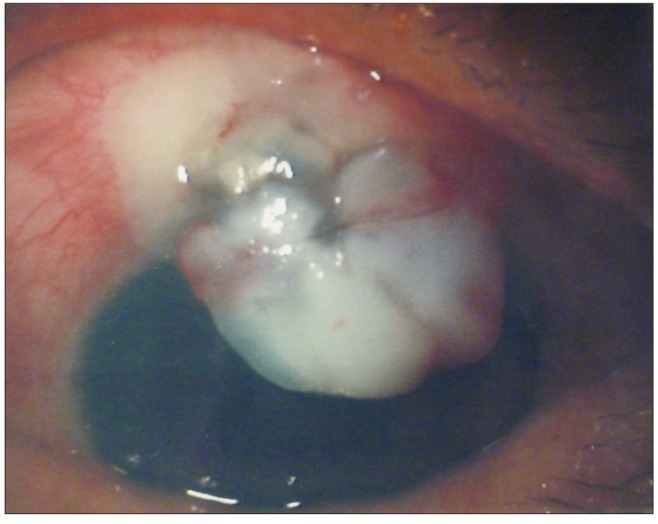
Indocyanine green (ICG) 0.25% (25 mg dissolved in 1 mL of aqueous solution, then into 9 mL of basic salt solution) was injected into the overhanging portion of the cystic bleb using a 30-guage needle. The ICG remained predominantly in the overhanging portion and did not extend to the superior portion of the bleb. A tourniquet was placed around an arm by an assistant and 1 mL of blood was withdrawn from the antecubital vein using a 5 mL syringe with a sterile 25-gauge needle. The surgeon held a 1 mL syringe with another 30-gauge needle and withdrew blood from the assistant's syringe. Autologous blood was gently injected into the overhanging portion of the bleb. An 8-0 Vicryl stitch was placed over the horizontal boundary between the overhanging and original portions of the bleb with the spatulated needles passing through partial-thickness of cornea just anterior to the limbus on both sides adjacent to the overhanging bleb (Fig. 3).
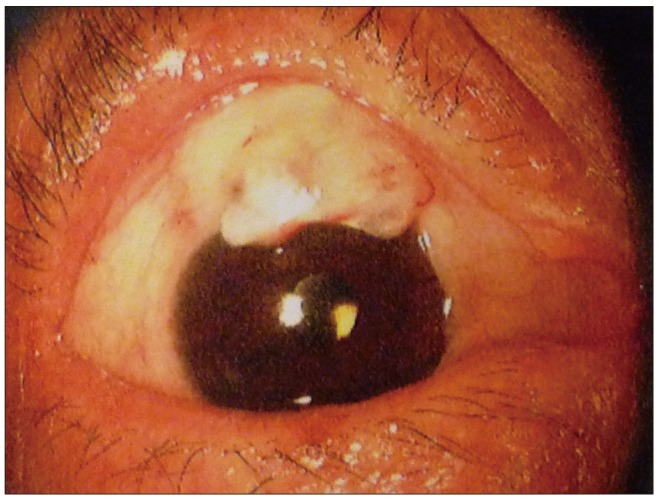
Blood remained in the overhanging portion of the bleb and no hyphema was observed in the immediate post-operative period. The IOP was maintained in the low teens and the overhanging portion slightly reduced in size and appeared more firm, due to fibrosis, over time. The patient deferred a second operation until 6 weeks later, and partial excision of the overhanging portion of the bleb was performed. Injection of ICG was attempted, but failed as the overhanging portion of the bleb was very firm due to fibrosis. The anterior border of the bleb was elevated from the cornea with a Took's knife, followed by excision of the overhanging portion with Wescott scissors. The compression stitch was removed and no leak was evident from the edge. The patient's best corrected visual acuity returned to 20 / 40 at 3-month follow-up (Fig. 4). IOP was maintained in the low teens, and the bleb remained well situated without exuberance throughout 9 months of follow-up.
Discussion
An overhanging cystic bleb has multi-loculated cystic structures covered with conjunctival epithelium [1]. It lies on the surface of Bowman's layer, which can be dissected off the underlying cornea [2]. It is an uncommon complication after glaucoma filtration surgery, with and without anti-metabolite therapy, and in both fornix- and limbal-based trabeculectomy [1-9]. The indications for intervention include overfiltration leading to hypotony, foreign body sensation, lid retraction, lagophthalmos, and compromised visual acuity. The aim of intervention is reduction of the exuberant tissue without compromising its excellent drainage function. Case series have described various approaches in management of overhanging cystic blebs, including cryotherapy [3], argon laser [4] and neodymium: YAG laser [5]. However, these procedures are not free of complications. These have been associated with bleb leaks, transient increase in IOP, corneal edema, and bleb failure, especially in eyes which had undergone previous filtration surgery with anti-metabolites. Two prior case series reported high success rates using an iris spatula to lift the bleb above the cornea with excision; however, these were prior to the popular use of anti-metabolites in filtration surgery [6,7]. Filtration blebs following anti-metabolite use are extremely thin and friable, and surgical manipulation may amplify the potential risk of bleb injury. Anis et al. [8] performed sutureless surgical revision in 6 eyes with symptomatic overhanging blebs after trabeculectomy with mitomycin C. A bandage contact lens was placed for 2 weeks postoperatively to enable re-epithelialization of the cut edge of the bleb at the limbus, however, 1 eye had a persistent bleb leak, requiring secondary suture repair. A conjunctival advancement flap with relaxing incision after partial excision of an overhanging cystic bleb following anti-metabolite trabeculectomy surgery has been reported [9], but required greater surgical manipulation of the conjunctiva. Desai and Krishna [10] described the combination of compression sutures and surgical excision in a large overhanging bleb with prior anti-metabolite use. Compression sutures may help reduce fluid conductivity, allow bleb wall remodeling, and enable epithelial healing [10].
In the present case, ultrasound biomicroscopy revealed multiple loculated compartments separated by thin septa within the cystic bleb. A high risk of cystic bleb damage, leading to leakage and hypotony, was anticipated while planning for operation. Autologous blood provides a source of trophic factors that induce migration and proliferation of adjacent fibroblasts, thereby promoting healing within the bleb [11]. A combination of autologous blood injection with compression sutures has been performed in overfiltering and leaking blebs [12,13], which maximized remodeling within the bleb and allowed for subsequent safe surgical removal.
Kim et al. [14] performed noninvasive preoperative examination of an overhanging cystic bleb using anterior segment optical coherence tomography and demonstrated images of the multi-loculated cystic structures in the dissecting portion of the bleb, subsequently removed without leakage. The multiple septate structures may have suppressed aqueous flow and prevented leakage after excision. Nevertheless, intra-operative damage to the main portion of the bleb is plausible, and injection of ICG clearly demonstrated the boundary between the overhanging and original portion of the bleb. Ito et al. [15] demonstrated the safety of ICG injection to visualize internal bleb structures prior to surgical removal of overhanging portions of cystic blebs. Autologous blood and compression suturing was effective in causing fibrosis within the overhanging portion, further ensuring that the original portion was completely sealed and its excellent filtration function was preserved. Hyphema has been reported as a complication associated with intra-bleb autologous blood injection. We did not observe spillover of ICG into the original portion of the bleb or into the anterior chamber prior to injecting autologous blood. Subsequent surgical excision of the overhanging portion was easy and safe, which alleviated the patient's foreign body sensation, and restored vision.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






