Kimura Disease Involving a Caruncle
Article information
Abstract
A 35-year-old woman presented with history of a painless, slow-growing nodule in a left eye caruncle over the last 2 months. The visual acuity was 20 / 20 and the ocular movements were in the normal range. The venereal disease research laboratory test, erythrocyte sedimentation rate, serum angiotensin converting enzyme level, and chest radiograph were all normal. An excisional biopsy was done to confirm the diagnosis. A 1.3 × 0.5 × 0.3 cm sized nodule was extracted and sent for histopathologic examination. Hematoxylin-eosin staining showed follicular hyperplasia with perifollicular fibrosis, an eosinophil infiltrate, and proliferation of capillary vessels. The capillaries were lined by normal-appearing, flat, spindle-shaped endothelial cells. On the basis of these histopathologic findings, the diagnosis of Kimura disease in a caruncle was established. This is the first report describing Kimura disease localized to a caruncle. Kimura disease should be suspected and included in the differential diagnosis of a caruncular mass lesion.
Kimura disease is a rare, chronic inflammatory disorder that usually involves the subcutaneous tissues and lymph nodes in the head and neck region of young Asian males [1-5]. This condition is a benign disorder of unknown etiology and may clinically simulate a neoplasm. Kimura disease has been reported to involve the oral cavity, axillae, groin, limbs, and trunk [3,4]. However, orbital, eyelid, and extraocular muscle involvement in Kimura disease is unusual [5,6]. We report the first case of Kimura disease involving a caruncle as confirmed by histopathologic examination in a middle-aged Asian woman.
Case Report
A healthy 35-year-old woman presented with a history of a painless, slow-growing nodule in the left eye caruncle over the previous 2 months (Fig. 1). On examination, neither proptosis nor ptosis was noted. The lesion was not fixed to the underlying tissue, was freely mobile, and had a firm consistency. Eversion of the upper and lower eyelids revealed that the lesion was confined to the caruncle without extension to the fornix or palpebral conjunctiva. The visual acuity was 20 / 20 and ocular movement was in the normal range. The ocular examination was otherwise unremarkable. On physical examination, there was no regional lymphadenopathy.
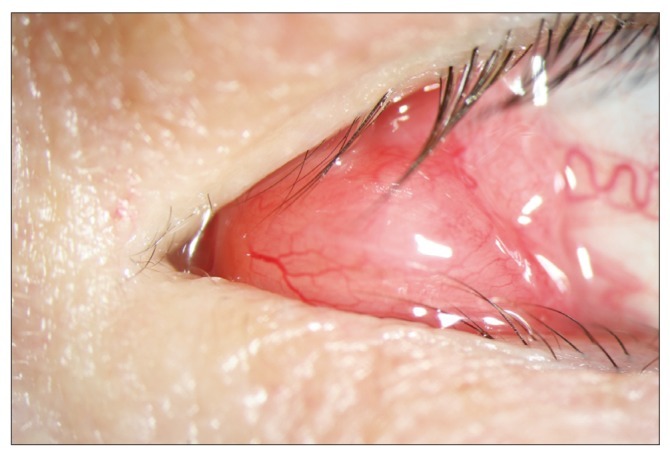
A slit lamp biomicroscopic finding on the patient's initial visit revealed a conjunctival nodule in the left medial canthal area.
The complete blood cell count was within the normal range. The venereal disease research laboratory test, erythrocyte sedimentation rate, serum angiotensin converting enzyme level, and chest radiograph were all normal. The serum IgE level was not elevated. Microalbuminuria was present. She had no prior significant medical history; however, she declined additional work-up.
One week following presentation, the patient underwent an excisional biopsy of the left eye to confirm the diagnosis. A 1.3 × 0.5 × 0.3 cm sized nodule was removed and subsequently sent for histopathologic examination. Gross examination of the mass revealed a smooth, firm nodule; infiltration to the underlying tissues was not detected. Microscopic examination with hematoxylin-eosin staining showed follicular lymphoid hyperplasia with germinal center and perifollicular fibrosis (Fig. 2). Higher magnification revealed an eosinophil infiltrate with proliferation of vascular channels, especially the capillaries (Fig. 3). Vascular channels were lined by normal-appearing flat, spindle-shaped endothelial cells (Fig. 4). Immunohistochemical staining for CD20 and CD3 showed T-cells surrounding well-formed lymphoid follicles with germinal centers containing B-cells (Fig. 5A and 5B).
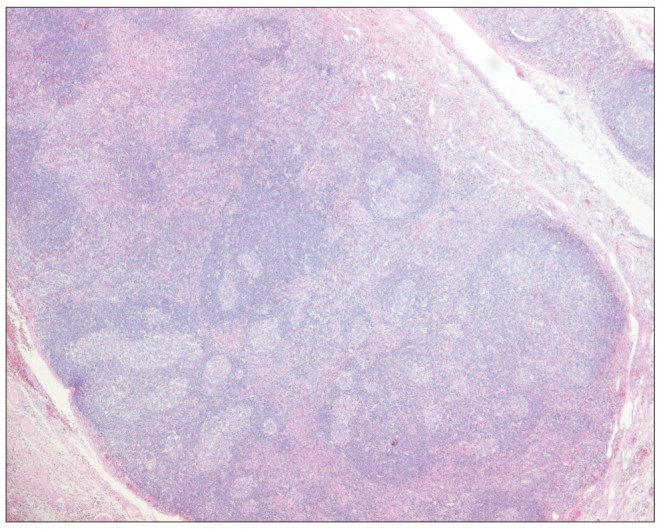
Histological findings of mass lesion (hematoxylin-eosin stain, ×100). Chronic inflammation with multiple follicular lymphoid hyperplasia with nodal germinal center.

Numerous infiltrated eosinophils with fibrous septa (hematoxylin-eosin stain, ×400).
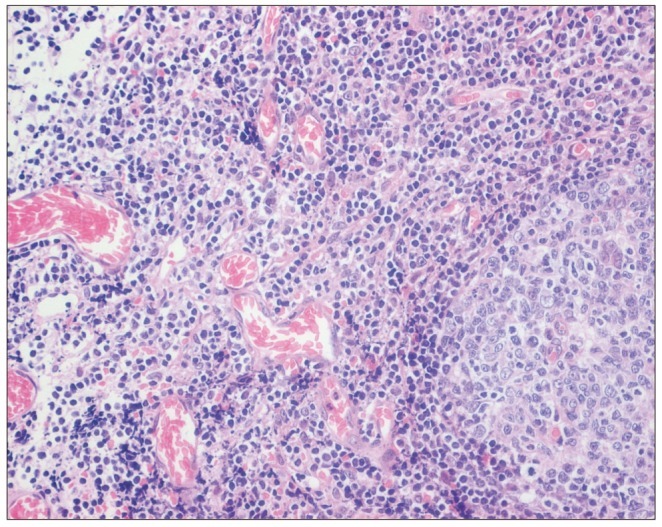
Multiple capillary proliferation with normal flat, spindle-shaped vascular endothelium (hematoxylin-eosin stain, ×400).
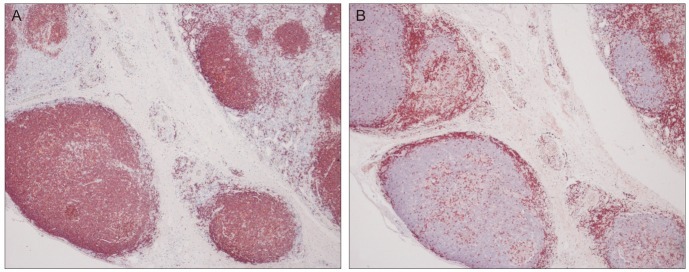
Immunohistochemical staining for CD20 and CD3 in Kimura disease (×200). The germinal center B-lymphocytes of follicles is positive for CD20 (A) and CD3 stained in the surrounding mantle zone of T-lymphocytes (B).
On the basis of these histopathologic findings, we established a diagnosis of Kimura disease. At the last follow-up 6 months after surgery, the patient had no evidence of a recurrence.
Discussion
The caruncle is a modified cutaneous tissue containing fine hair, sebaceous glands, sweat glands, and goblet cells [7]. Although this large array of tissue elements can give rise to a wide variety of lesions, caruncular tumors are uncommon [7]. This is the first report describing Kimura disease localized to a caruncle. Kimura disease typically presents as firm, painless, pruritic, single-to-multiple subcutaneous nodules [4]. Kimura disease has a predilection for the skin of the pre-auricular, parotid, and submandibular regions. Kimura disease of the orbit and ocular adnexa is uncommon, but well-documented by Buggage et al. [5]. The orbit, especially in the superior orbital space, may be a preferred site for Kimura disease. The disease was first described in Chinese literature as an eosinophilic hyperplastic lymphograuloma and was later characterized by Kimura et al. in 1948 [1]. Hundreds of cases under a variety of names have been reported in Asia, including China, Japan, and Indonesia.
Kimura disease occurs mainly in Asian males, presenting as large (>2 cm) subcutaneous papules or nodules, elevated blood eosinophilia (up to 54%), hypergammaglobulinemia (IgE), regional lymphadenopathy, and salivary gland involvement [8,9]. Systemic symptoms (fever, night sweats, and weight loss) are uncommon. The patient described herein was female and had a normal peripheral blood eosinophil count and serum IgE level.
The etiology and pathogenesis of Kimura disease are unknown. Allergic reactions, infections, and autoimmune reactions with an aberrant immune response have been suggested [10]. Because of the non-specific presentation of Kimura disease, strict histopathologic examination is crucial to confirming the diagnosis. Histopathologically, Kimura disease is characterized by an inflammatory infiltrate with prominent collections of eosinophils and scattered lymphoid follicles, increased fibrocollagenous tissue, and vascular proliferation, with vessels lined by normal endothelial cells [11]. Our case also showed the typical pathologic findings which occur in Kimura disease.
The differential diagnosis of Kimura disease is broad and includes angiolymphoid hyperplasia with eosinophilia (ALHE), Hodgkin lymphoma, Langerhans cell histiocytosis, lymphadenopathy of a drug reaction, and parasitic lymphadenitis. However, distinguishing Kimura disease from neoplasms is not difficult when Reed-Sternberg cells, atypical lymphocytes, and Langerhans cells are identified. A positive history of drug use, and seropositivity for parasitic infections can be helpful for differentiating diagnoses.
Kimura disease and ALHE were often confused in a number of early reports [5,11]. Over the years, the clinical features of Kimura disease overlap significantly with those of ALHE. Clinically, both present as relatively asymptomatic soft tissue swellings in the head and neck. However, there are characteristic and distinctive clinicopathological features between the two diseases. In brief, Kimura disease occurs predominantly in Asian males. Patients mostly demonstrate a peripheral eosinophilia and elevated serum IgE levels. The solitary lesions are usually in the deep subcutaneous tissues, and are frequently associated with regional lymphadenopathy and salivary gland involvement. By contrast, ALHE occurs in all racial groups with a slight female predilection. Patients present with small, superficial dermal papulonodules, which are frequently erythematous, accompanied by bleeding, pruritis, and tumor growth. Regional lymphadenopathy, serum eosinophilia, and elevated IgE levels are rare [11]. Kimura disease and ALHE can be differentiated on a histopathological basis, especially with their vascular endothelial morphology. Kimura disease is a chronic allergic or autoimmune inflammatory disorder, whereas ALHE is a neoplasm of blood vessels [10]. Histopathologically, the most important diagnostic feature of ALHE is the appearance of endothelial cells, which have a vesicular nucleus, abundant cytoplasm, and an oval-to-cuboidal shape [5]. These endothelial cells can project into vascular spaces or form deposits in vessels [5,12,13]. Stromal fibrosis is uncommon in ALHE [8]. In our patient, the histopathologic examination of the surgical specimen revealed flat, spindle-shaped endothelial cells which had normal-appearing nuclei and cytoplasm; findings which are consistent with Kimura disease.
Interestingly, Kimura disease is associated with renal disease, which may develop before or concurrently with disease progression [14]. Googe et al. [8] demonstrated IgE in the renal glomeruli of a patient with Kimura disease who manifested nephritic syndrome. Our patient had microalbuminuria, but declined additional work-up.
The optimal treatment for Kimura disease has not been determined. Excision is the most widely used therapy and oral or intralesional steroids, radiation, and chemotherapy can also be used. Recurrence after excision is common because of incomplete excision [3]. Considered an inflammatory process, the disease has an excellent prognosis. We treated the patient with complete excision and recurrence has not been detected through the 6-month follow-up visit.
There is a tendency for caruncular lesions to have inconsistencies between clinical and histopathologic diagnosis, which can be as high as 50% [15]. Our patient is a further unusual example of the confounding nature of the caruncular lesions. Despite its rarity, Kimura disease should be included in the differential diagnosis of caruncular lesions. Caruncular lesions are rare and diverse, making clinical diagnosis difficult. With a strict histopathologic examination of excised tissue, a correct diagnosis can be achieved.
Notes
No potential conflict of interest relevant to this article was reported.