

For chronic paralytic strabismus with large eyeball deviation, there are only a few surgical options including recession-resection surgery and muscle transposition. Given that full tendon transposition (FTT) augmented with posterior scleral fixation suture is very effective but complicated, FTT augmented with a posterior intermuscular suture (PIMS) has been suggested [1]. However, even for strabismus specialists, FTT with PIMS is somewhat complicated. We considered a recession-resection surgery reinforced with botulinum toxin A chemodenervation as another surgical option for chronic paralytic strabismus with large deviation.
Here, we compare the effects of recession-resection surgery augmented with botulinum toxin A chemodenervation with those of FTT augmented with PIMS for patients with chronic paralytic horizontal strabismus.
Case Reports
Case 1
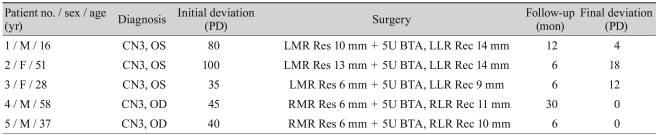
A 16-year-old man had a history of radiotherapy for astrocytoma. He had left exotropia of 80 prism diopters (PD) and left hypertropia of 10 PD. He had a loss of left adduction, and there was no midline cross. A recession-resection procedure of the horizontal recti muscles with inferior displacement was planned for the paralytic eye. A left lateral rectus recession of 14.0 mm and left medial rectus resection of 10.0 mm, combined with intraoperative injection of five units botulinum toxin A into the left lateral rectus, were performed. One year later, the patient was found to have left esotropia of 4 PD and left hypertropia of 6 PD in the primary position. No additional procedure was necessary.
Case 2
A 58-year-old man had chronic right third cranial nerve palsy caused by a pituitary gland tumor. A dilated, fixed pupil was observed in his right eye. He had right exotropia of 45 PD and right hypertropia of 4 PD. Right lateral rectus recession of 11.0 mm and right medial rectus resection of 6.0 mm with inferior displacement, combined with intraoperative injection of 5 units botulinum toxin A into the right lateral rectus, were performed. At a 30-month follow-up, the alignment was nearly straight in the primary position at near and far distances.
We retrospectively reviewed the medical records of five patients who received a recession-resection surgery augmented with botulinum toxin A chemodenervation (type I surgery) from January 1998 to December 2007. These patients had third cranial nerve palsy with exotropia. All surgical procedures were performed by a strabismus specialist, and the same investigator obtained all the pre- and postoperative data. During surgery, five units of botulinum toxin A (Botox; Allergan Inc., Irvine, CA, USA) in 0.1 mL of saline solution was injected into the recessed horizontal rectus muscle after conventional recession-resection. The injection was administered slowly under direct visualization.
We compared the results with those of FTT augmented with PIMS (type II surgery). According to the type of procedure, the pre- and postoperative angles of deviation (AOD) were compared.
Tables 1 and 2 provide a summary of the patient characteristics. The mean ages of the type I and type II surgery groups were 38.00 ± 16.99 years and 41.00 ± 10.39 years (range, 16 to 58 years), respectively. The mean follow-up time for all patients was 11.00 ± 8.76 months (range, 6 to 30 months).
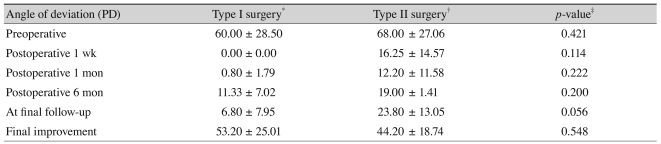
The data on pre- and postoperative AOD are shown at Table 3. The mean preoperative AOD was 60.00 ± 28.50 PD (type I surgery) and 68.00 ± 27.06 PD (type II surgery) (p = 0.421). At preoperative and postoperative 1 week, 1 and 6 months, and the final follow-up, the AODs were not significantly different. In addition, the final improvement in AOD was 53.20 ± 25.01 PD (type I surgery) and 44.20 ± 18.74 PD (type II surgery) (p = 0.548). There were no complications such as a scleral perforation, anterior segment ischemia, or ptosis in any of the cases during the surgical procedure or in the postoperative follow-up period. All statistical analyses including the Mann-Whitney U-test were performed with SPSS ver. 15.0 (SPSS Inc. Chicago, IL, USA).
Discussion
The surgical goal for chronic paralytic strabismus is to center the field of single binocular vision and to align the eyeballs in primary and down-gaze positions. Although the surgical choice usually depends on the amount of residual muscle function, a large recession-resection surgery or transposition of recti muscles may be selected.
Previously, Ozkan et al. [2] reported the effect of intraoperative botulinum toxin A injection combined with conventional horizontal recti muscle surgery in ten patients with infantile esotropia, nonrefractive accommodative esotropia, partial accommodative esotropia, basic esotropia, basic exotropia, and sensory exotropia.
According to neurophysiological studies, botulinum toxin A applied to the periphery could directly affect central circuits via retrograde transport [3]. In addition to preventing muscle contracture, botulinum toxin A injection causes permanent alteration in the muscle and influences the peripheral and central nervous systems. Kranjc et al. [4] studied the long-term changes of extraocular muscles after botulinum toxin A injection into the medial rectus muscles of adult rats. These changes occurring in the horizontal rectus muscles after botulinum toxin A chemodenervation may be responsible for the permanent additive effect of botulinum toxin A.
In our cases, the patients had large exotropia with chronic third cranial nerve palsy. There was a loss of adduction and no midline cross. We performed simple recession-resection surgery accompanied by intraoperative botulium toxin A chemodenervation. Our results show that a recession-resection surgery augmented with botulinum toxin A chemodenervation had a similar effect to that of FTT augmented with PIMS. Even though FTT augmented with PIMS is relatively simple and safe compared to other surgeries for chronic paralytic strabismus with large deviation, it may be technically more difficult than a recession-resection surgery. Thus, our recession-resection surgery augmented with botulinum toxin A chemodenervation technique is a good surgical option. However, due to the small number of patients, the present study has limited statistical validity. Well-designed prospective studies are needed to compare botulinum toxin A treatment to standard surgical management.
In conclusion, the recession-resection surgery augmented with botulinum toxin A chemodenervation is as effective as FTT augmented with PIMS for treating paralytic horizontal strabismus.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






