

Peters' anomaly is characterized by central corneal opacity with defects in the corneal endothelium, Descemet's membrane, and posterior stroma. Variable degrees of iridolenticulocorneal adhesions are often also present [1]. Peters' anomaly may be isolated or accompanied by other ocular malformations such as chorioretinal coloboma, a congenital defect caused by faulty closure of the embryonic fissure, and associated with other ocular and systemic abnormalities [2]. Here, we describe a case of unilateral Peters' anomaly in the left eye and chorioretinal coloboma in the right eye.
Case Report
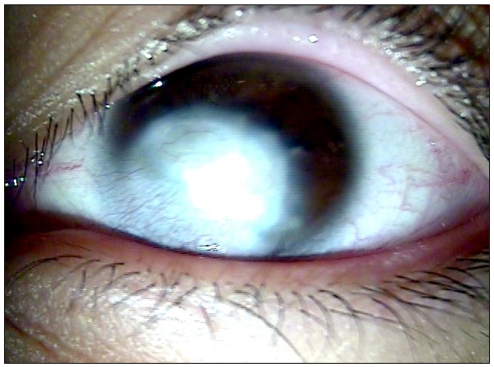
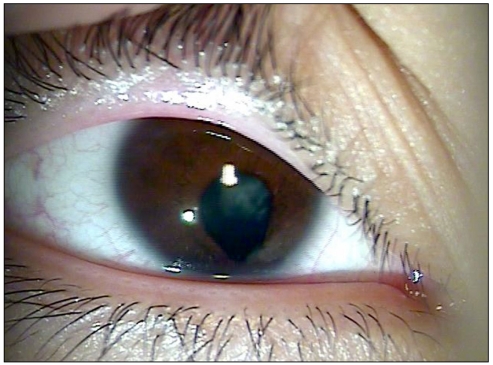
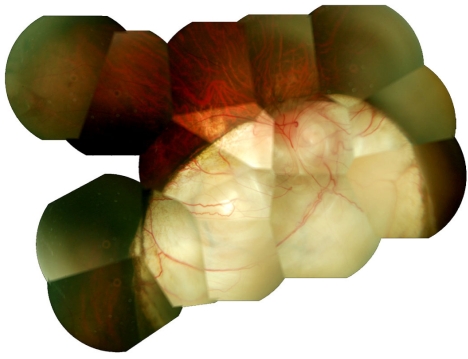
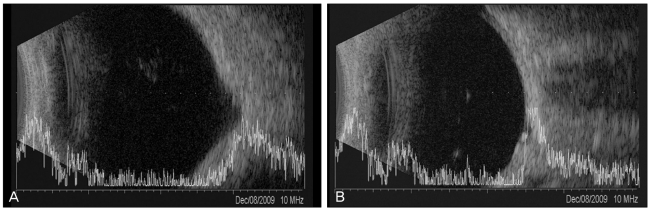
An 18-year-old man presented with poor vision in both eyes that had been present since birth. On presentation, his visual acuity was 60 / 200 in the right eye and light perception only in the left eye. The refractive error in the right eye was -11.0 diopters, and we were unable to measure the refractive error of the left eye because of sclerocornea. Intraocular pressure was 27 mmHg in the right eye and 21 mmHg in the left eye. Central corneal opacity and inferior peripheral sclerocornea with iridocorneal adhesion were observed in the anterior segment of the left eye (Fig. 1). The right eye had an iris coloboma that manifested as a small notch in the inferior pupillary margin and cataract (Fig. 2). Fundus examination of the right eye showed a large inferior chorioretinal coloboma involving the optic disc and macula (Fig. 3). Staphyloma was observed in the right eye by B-scan ultrasonography (Fig. 4A). We did not detect any systemic malformations and there was no relevant family history.
Discussion
Since Peters' original description in 1906 [3], many others have reported ocular abnormalities now known as Peters' anomaly. The causes of Peters' anomaly are unknown; it may be caused by genetic factors, environmental factors, or both. Peters' anomaly displays various patterns of inheritance, either autosomal dominant or autosomal recessive, but cases of autosomal dominant Peters' anomaly are rare [4].
The PAX6 gene, which is expressed in the developing central nervous system including the eye, has been shown to be vital to eye development and to be influential at early stages of ocular morphogenesis, acting as a master control gene [5]. It is therefore believed to play an important role in ocular embryogenesis. Mutations in the PAX6 gene are associated with various ocular anomalies, including Peters' anomaly, aniridia and chorioretinal coloboma [6]. We did not perform genetic analyses of our patient. Genetic studies of the patient and his relatives may help to elucidate the causes of this anomaly.
Our patient also had chorioretinal coloboma in the right eye. Retinal detachment is the most common complication associated with chorioretinal colobomas, due to breaks within or adjacent to the coloboma. The retina overlying the choroidal defect in such cases remains thin and undifferentiated and, therefore, prone to retinal breaks and detachment. Most retinal detachments associated with chorioretinal coloboma require surgery and have poor visual outcomes. Forty percent of affected individuals may develop retinal detachment during their lifetimes [7-10]. Therefore, it is important to examine the fundus in detail, if possible, in patients who are diagnosed with Peters' anomaly to detect any associated congenital anomalies such as chorioretinal coloboma. It is recommended to examine eyes affected by chorioretinal coloboma at least annually to prevent complications such as retinal detachment. To our knowledge, this is the first documented case of unilateral Peters' anomaly with chorioretinal coloboma in the other eye in Korea.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






