Evaluation of the Central Macula in Commotio Retinae Not Associated with Other Types of Traumatic Retinopathy
Article information
Abstract
Purpose
To report on the anatomical and functional changes to the macula in nine patients suffering from commotio retinae not accompanied by any other types of traumatic retinopathy.
Methods
Nine injured eyes with commotio retinae were evaluated soon after ocular trauma with ophthalmic examination, including Spectral-domain optical coherence tomography (SD-OCT). In 12 eyes of 6 patients, Humphrey visual field (HVF) and multifocal electroretinogram (mfERG) were performed. Re-examinations were periodically performed for a mean of 26 days. Data from 9 injured eyes were collected and compared to data collected from the 9 non-affected eyes of the same patients.
Results
SD-OCT revealed no significant differences in the foveal thickness and total macular volume between traumatized and intact eyes in all 9 patients. Only 3 out of the 9 injured eyes showed abnormal findings in SD-OCT images such as discontinuity of the inner/outer segment (IS/OS) junction or abnormal hyper-reflectivity from the IS/OS and retinal pigment epithelium (RPE) lines in the macula. HVF and mfERG results did not show any functional deterioration in the injured eyes compared with intact eyes. During follow-up, the commotio retinae resolved in all 9 eyes. The changes to the outer retinal region detected in 3 patients by SD-OCT were also resolved.
Conclusions
Acute retinal changes in commotio retinae, not associated with other retinal pathologies, were resolved without histological and functional sequelae. In a few cases of commotio retinae, SD-OCT revealed transient abnormalities mainly observed at the IS/OS and RPE complexes.
Commotio retinae, a condition caused by a direct ocular injury, was first described by Berlin in 1873 [1] and when it involves the macula it is called Berlin's edema. Commotio retinae is characterized by a transiently whitish coloration which is comparatively well-defined on the retina.
There have been a few histological studies into why a whitish coloration occurs [2-4]. Berlin suggested that the whitish coloration might occur due to extracellular edema [1]. In recent reports however, extracellular edemas were not observed [2-4]. The disruption or fragmentation of the photoreceptor outer segment (OS) of the retina is the most common finding in histological studies of commotio retinae [2-4].
As an alternative to traditional histology, optical coherence tomography (OCT) provides a cross-sectional structure of the retina, allowing the observer to see each layer while providing detail comparable to a histological section. The technologic advancement of OCT thus makes it possible to describe the retinal anatomy in place of histological studies. Recently, OCT has been applied to the pathophysiological analysis of commotio retinae, resulting in confirmation of previous histological studies of the abnormality of the retina outer segment layer [5,6]. Furthermore, spectral-domain (SD)-OCT allows in vivo visualization of intraretinal structure, especially the retinal pigment epithelium (RPE), inner segment (IS) and OS of the photoreceptor layer, all of which are involved in commotio retinae.
In this study, we focused on patients with commotio retinae involving the fovea and not accompanied by other types of trauma-related retinal conditions. Structural and functional analyses were performed through SD-OCT, a visual field test and multifocal electroretinogram (mfERG).
Materials and Methods
Described herein is a retrospective study of clinical findings from a series of 9 eyes belonging to 9 patients with Berlin's edema, all referred to the department of ophthalmology, between December 2009 and March 2010. Eight patients were male and 1 patient was female. All patients provided informed consent after getting a full explanation of the examinations. Institutional review board of approved this study. Patients were first examined on the day of or within 3 days after the trauma and observed only with conservative management for a mean of 26 days (range, 2 to 88 days). All cases exhibited a white opaque zone in the central macula following blunt trauma and did not exhibit other retinal abnormalities such as preretinal, retinal, or subretinal hemorrhages, choroidal rupture, macular detachments, or partialor full-thickness macular holes. All patients underwent a complete ophthalmic examination, including history, slit-lamp biomicroscopy with or without a noncontact fundus lens (SuperField lens; Volk Optical Inc., Mentor, OH, USA), best corrected visual acuity, fundus photography, and SD-OCT (Cirrus HD-OCT; Carl Zeiss Meditec Inc., Dublin, CA, USA) with 5 µm of axial resolution and 10 µm of horizontal resolution.
To evaluate any change in the retinal thickness and sub-/intra-retinal abnormalities at the traumatized central macula, we compared foveal thickness and total macular volume between the affected and non-affected eye using a macular cube scan. We also evaluated the integrity of the reflective line of the photoreceptor IS/OS and RPE from the 5-line raster scan and the macular cube scan. The correct alignment of the testing cube (6 × 6 mm) was confirmed at each examination.
To analyze potential functional changes due to the whitish opaque foveal lesions, a visual filed test and mfERG were performed in 6 selected cases (cases 4-9). Automated perimetry was performed with a Humphrey field analyzer II (model 750; Carl Zeiss Meditec Inc.) using the C30-2 program with the standard Swedish Interactive Algorithm protocol. Values of mean deviation (MD) were analyzed at the first visit, and if any significant changes were detected automated perimetry was rechecked at subsequent visits. A visual field was defined reliable when fixation losses, false positive, and false negative rates were less than 20% each. For mfERG recording, a visual evoked response imaging system (VERIS 4; EDI, San Mateo, CA, USA) was used. The patients' pupils were fully dilated with 0.5% tropicamide and 0.5% phenylephrine hydrochloride. After instillation of the topical anesthetic, Alcaine® (0.5% proparacaine), Burian-Allen bipolar electrode lenses were applied to the cornea. One hundred and three elements were used in the recordings. The Ring 1 response was recorded according to the guidelines for the basics of mfERG to assess any functional change to the fovea. The results from subjects were analyzed by Wilcoxon's signed rank test in SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA) and differences were considered to be significant when p < 0.05.
Results
Table 1 summarized the characteristics and ocular findings of the 9 patients. The age of patients ranged from 12 to 54 years old (mean, 22.5 years). Visual acuities ranged from 20 / 40 to 20 / 20 at the initial visit. No patients had anisometropia (>2.0 diopters [D]), extreme hyperopia (>+3.00 D) or myopia (<-6.00 D). In all 9 eyes the anterior segments were unremarkable, except for microscopic hyphema observed in the injured eye of case 4 and a mild traumatic iritis in the traumatized eye of case 8.
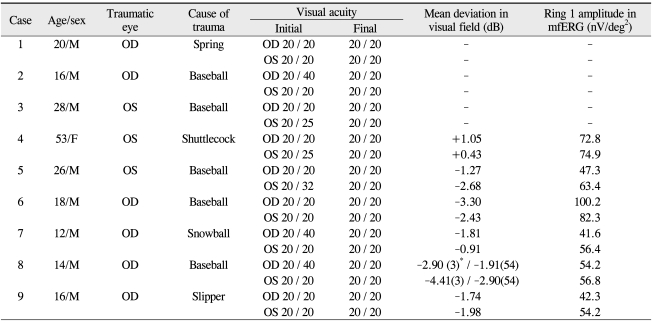
The characteristics and ocular findings of the patients
Humphrey automated visual field tests showed no significant changes (p = 0.463). A slightly decreased value of MD was observed in cases 7 and 8. Ring 1 amplitudes recorded from 6 of the patients did not reveal any significant differences between injured and normal fovea (p = 0.345) (Table 1).
Macular cube scans of the OCT revealed no significant differences of the foveal thickness (p = 0.307) or the total macular volume (p = 0.123) between traumatized and intact eyes in all 9 cases (Table 2). However, in 3 eyes of 3 patients, discontinuity of the IS/OS junction and abnormal hyper-reflectivity from the IS/OS and RPE lines were observed in the macula.
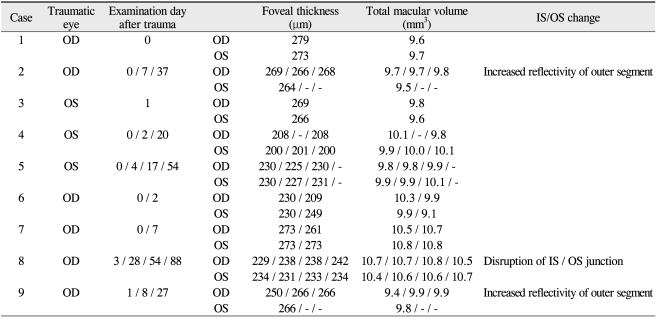
The spectral-domain optical coherence tomography findings of the patients
During a follow-up without management, the commotio retinae resolved gradually within 7 days in 8 eyes, and within 3 months in the rest of the eye. The changes of the outer retinal region detected in 3 patients by SD-OCT also resolved within 3 months.
Selected case reports
1) Case 2
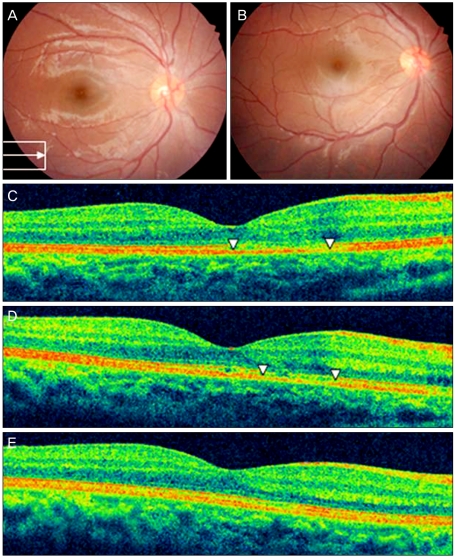
A 16-year-old male presented with blurred vision on his right eye after blunt injury by a baseball. On examination, Visual acuity was 20 / 40 in the right eye and 20 / 20 in the left eye. Both eyes' anterior segments were found to be normal by slit lamp biomicroscopy. Fundus examination showed a localized area of commotio retinae in the macula (Fig. 1A). The left eye was normal. OCT revealed loss of definition of alternate layers and unusual hyper-reflectivity in the area of the IS/OS and RPE complex (Fig. 1C and 1D). At 1 week after the injury, the commotio retinae resolved (Fig. 1B). Concomitant with the anatomic improvement, the visual acuity improved to 20 / 20. OCT demonstrated normalized reflectivity and well-demarcated alternate layers form the IS/OS and RPE complex (Fig. 1E and 1F) at that time.
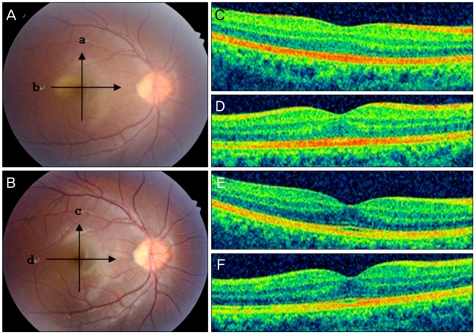
Case 2. (A) Fundus photograph showing retinal opacity on the day of trauma. (B) Fundus photograph at 7 days post-trauma showing resolution of commotio retinae. (C) and (D) are optical coherence tomography (OCT) images taken on the day of trauma, showing increased reflectivity in the area of the photoreceptor outer segment (these scans correspond to line scans a and b on A). (E) and (F) are OCT images taken 7 days post-trauma, revealing restoration to the normal alternated layer (these scans correspond to line scans c and d on B). Arrows denote the orientation of the OCT line scan.
2) Case 6
An 18-year-old male presented after experiencing blunt injury to his right eye by a baseball. At presentation, visual acuity of the right eye was 20 / 20 and the fundus examination showed a diffuse whitish opaque lesion in the posterior pole (Fig. 2A). OCT demonstrated normal alternated retinal layers of the IS/OS and RPE complexes in the macula (Fig. 2C). Both the response from the central retina by analysis with mfERG and the result of the visual field test were unremarkable and similar to data obtained from the unaffected eye. Follow-up by ophthalmoscopy revealed resolution of the commotio retinae (Fig. 2B) and OCT revealed unremarkable findings of the macula (Fig. 2D) by 2 days after the injury.
Case 6. (A) Fundus photograph and (C) optical coherence tomography, taken the day of trauma, revealing commotio retinae and anormal alternated layer. (B) and (D), taken 2 days post-trauma, showing resolution of the commotio retinae and unremarkable findings of the macula.
3) Case 8
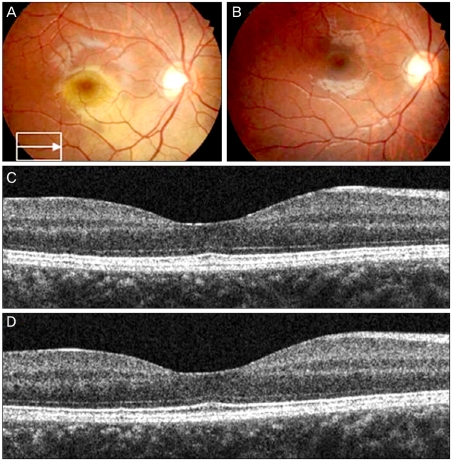
A 14-year-old male noted decreased central vision in his right eye after blunt injury by a baseball. He was referred to us 3 days after the trauma. The left eye was normal. At presentation, visual acuity of the right eye was 20 / 40 and a few cells were observed in the anterior chamber of the right eye. Fundus examination showed a small opacity on the macula (Fig. 3A). The response of mfERG from the central retina and the result of the visual field test were similar to data obtained from the unaffected eye. OCT demonstrated the discontinuity of the IS/OS junction at the corresponding area of the commotio retinae (Fig. 3C). At 10 days after the trauma, commotio retinae was still observed by indirect ophthalmoscopy. At 28 days after the trauma, visual acuity of the right eye was 20 / 25. Fundus examination revealed a partial regression of the retina opacity but still showed abnormal foveal reflex (data not shown) at this time.
Case 8. (A) Fundus photograph at 3 days post-trauma showed retinal opacity on the macula (arrow in the box denotes the orientation of the optical coherence tomography [OCT] line scan). (B) Fundus photograph at 54 days post-trauma revealing resolution of commotio retinae. (C) OCT scan at 3 days post-trauma showing the discontinuity of the inner segment/outer segment (IS/OS) junction at the corresponding area of the commotio retinae (arrow heads in C) (D) OCT scan at 54 days post-trauma demonstrate partial resolution of the discontinuity at the IS/OS junction (arrow heads in D). (E) At 88 days post-trauma, OCT revealed restoration of IS/OS junction.
A follow up observation by indirect ophthalmoscopy showed resolution of the commotio retinae by 54 days after the injury (Fig. 3B). At this time, the visual acuity of the right eye improved to 20 / 20. OCT demonstrated partial resolution of discontinuity at the IS/OS junction (Fig. 3D). At post-traumatic day 88, continuity of the intact IS/OS junction was almost restored but still showed an uneven reflectivity of the IS/OS junction (Fig. 3E).
Discussion
Commotio retinae is commonly seen after blunt trauma. It occurs in response to application of a blunt force to the eyeball causing a contrecoup injury characterized by transient retinal whitening. The goal of this study was to evaluate histological and functional changes of pure Berlin's edema not associated with any other traumatic retinopathies such as intra-/sub-retinal hemorrhages, choroidal rupture, traumatic macular hole, and so on.
Recently, Lai et al. [7] reported a case report showing mfERG changes in commotio retinae associated with traumatic macular hole. It was suggested that the permanent loss of retinal function following commotio retinae could be possible due to permanent loss of photoreceptors. However, in our observations no significant functional damages were detected either using the automated visual field test or the mfERG. The MD values of the Humphrey visual field tests in the injured eyes were not different from those from the contralateral uninjured eyes. Additionally, Ring 1 amplitudes of mfERG showed no differences between injured and normal fovea. This discrepancy of retinal responses measured by mfERG between Lai's and our studies could result from the different severity of the impact to the injured eyes. Retinas in cases of commotio retinae accompanied by other traumatic retinopathies are likely to have more severe damage than retinas exhibiting commotio retinae only. Therefore, it could be suggested that prognosis might be dependent not on the presence of commotio retinae itself, but on other associated retinal pathologies.
Observation of intraretinal details using high imaging quality and fine resolution is important for obtaining a better understanding of pure commotio retinae. OCT is a non-invasive technique that provides optical cross-sectional images of the retina and morphologic information close to that obtained from histological studies. Macular cube scans of SD-OCT revealed no significant differences of the foveal thickness and total macular volume between injured and uninjured eyes in all 9 cases. This result is consistent with previous reports demonstrating no extracellular edema histologically [2-4]. Among the 9 injured eyes exhibiting whitish opaque changes at the fovea upon the fundus examination, 3 eyes showed abnormal findings in the SD-OCT, while the rest of the cases revealed normal reflectivity in the OCT regardless of the commotio retinae.
Standard time-domain OCT, which was used in the previous studies of commotio retinae, enables visualization of the intraretinal structure [5,6]. However, this imaging does not have the resolution necessary to clarify the detailed features of the photoreceptor layer. SD-OCT has enabled improved visualization of the intraretinal morphology, allowing for examination of the external limiting membrane and the IS/OS junction. The IS/OS junction appears as a defined line due to the consistent thickness of the outer segment between photoreceptor cells in the normal macula. Therefore, loss of integrity in the IS/OS junction seen with SD-OCT could result from both reversible changes of photoreceptor outer segments and irreversible photoreceptor death. Mansour and associates [4] used histopathology to demonstrate that commotio retinae was associated with photoreceptor outer segment disruption. In the 9 cases of commotio retinae observed here, 8 eyes support this previous report. Whitish opaque retinal lesions disappeared within 1 week and among those, only 2 eyes demonstrated abnormal hyper-reflectivity of the IS/OS and RPE complex at the fovea. As previously suggested, these inconsistent OCT findings detected in the acute phase resulted from the variable severities of the physical impact to the retina.
On the other hand, more critical damage to the inner segment and the cell body of the photoreceptor itself were also described in animal models of commotio retinae [8]. OCT finings of case 8 can be explained with these previous reports; restoration of the discontinuous IS/OS junction was not complete until almost three months after the initial injury. Thus, commotio retinae is thought to involve more than the outer segments of the photoreceptor in case 8.
This study has limitations, especially with regard to the relatively small sample size. However, it was consistently observed that commotio retinae not otherwise associated with other traumatic retinopathies was not associated with significant functional changes to the retina and those histological abnormalities observed were fully resolved. This differs from previous case reports describing complicated commotio retinae [5-7]. SD-OCT may be a useful method to identify the gradual changes of the central retina with commotio retinae, providing accordance with histological data. In conclusion, when commotio retinae was the sole retinopathy found upon fundus examination, OCT demonstrated normal retinal structure or transient abnormalities mainly observed at the IS/OS and RPE complex.
Notes
No potential conflict of interest relevant to this article was reported.