

Congenital aniridia is a rare ocular malformation that affects the development of multiple ocular structures, this abnormality is caused by a mutation in the PAX6 gene located on chromosome 11p13 [1-3]. Iris hypoplasia is the most obvious sign, but a broad spectrum of disorders can manifest from various mutations in the PAX6 gene [2-4]. Many patients develop corneal opacities, cataracts, nystagmus, and foveal and optic nerve hypoplasia. Aniridia typically causes severe visual impairment; foveal hypoplasia is a major factor that can decrease visual function in these patients [5].
The incidence of congenital aniridia ranges from 1:64,000 to 1:96,000 [5]. In 2/3 of cases the abnormality is inherited in an autosomal dominant fashion with almost complete penetrance and variable expressivity, 1/3 of the cases of aniridia are sporadic [1,6,7].
The aim of this study was to investigate the clinical features of Korean patients with congenital aniridia. We analyzed the influence of treatment on the accompanying complications to determine the visual prognosis and assess disease progression.
Materials and Methods
This retrospective study focused on Korean patients who were diagnosed with congenital aniridia at Kangnam St. Mary's Hospital from 1996 to 2007. All cases were bilateral; however, 2 patients had already developed phthisis bulbi in one eye. We therefore included 60 eyes from 31 patients.
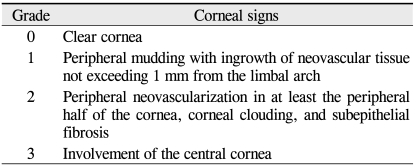
The age, gender, visual acuity (VA), family history, and previous ocular history of the patients were recorded. A thorough slit lamp microscopic examination was performed. The sporadic cases were diagnosed with typical clinical features of congenital aniridia without a positive family history. The presence or absence of keratopathy, glaucoma, cataract, and foveal hypoplasia were evaluated in each patient at the initial visit. Patients with uncontrolled intraocular pressure or a glaucomatous optic disc were regarded as having glaucoma. The extent of corneal involvement was classified into four grades (Table 1). The central corneal thickness was measured with an ultrasonic pachymeter (AL-2000; Tomey, Erlangen, Germany). Specular microscopy was performed using a non-contact Konan specular microscope (Robo Ca; Konan, Hyogo, Japan). The intraocular pressure was measured with Goldmann's applanation tonometry and a Tonopen.
Statistical analysis was performed using the t-test with SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered statistically significant.
Results
Patient demographics
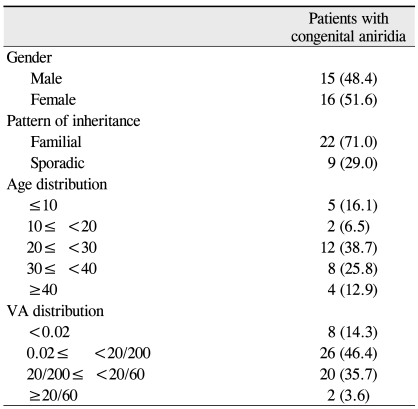
Table 2 shows the demographic data of the 60 eyes from 31 patients at the initial visit. The male/female ratio was 0.48. The proportion of sporadic cases was 29.0%. The mean patient age at the initial visit was 27.5 ┬▒ 9.6 years (range, 0.1 to 52 years). The majority of the patients were in their twenties (38.7%) and thirties (25.8%). Common chief complaints included a progressive decrease in VA due to cataract or keratopathy and uncontrolled intraocular pressure.
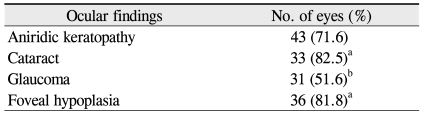
More than half of the patients had VAs less than 20/200 (Table 2). Twenty eyes (35.7%) had VAs between 20/200 and 20/60. Only two eyes from 1 patient had VAs better than 20/60. In addition to iris involvement, cataract (82.5%), glaucoma (51.6%), keratopathy (71.6%), and foveal hypoplasia (81.8%) were also observed (Table 3). The mean grade of keratopathy in 22 eyes with VAs better than 20/200 was 1.62 ┬▒ 0.89, which was statistically significantly lower than that in 34 eyes with VAs < 20/200 (2.38 ┬▒ 1.02, p = 0.035).
Aniridic keratopathy
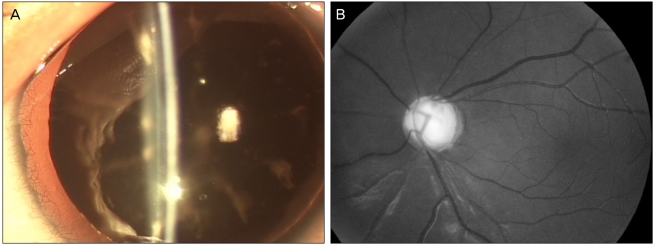
Various degrees of corneal opacities were found in 43 eyes (71.6%). Partial mudding in the peripheral limbal cornea with in-growth of vessels was regarded as grade 1 aniridic keratopathy (Table 1 and Fig. 1B) [8,9].
In children under the age of 10 years, 5 eyes had relatively clear corneas. Grade 1 keratopathy was found in 3 eyes from 2 patients who were treated for congenital glaucoma and grade 3 keratopathy was observed in 2 eyes. Grade 1 keratopathy was found in all 4 eyes from 2 patients who were in the second decade of life.
In 35 eyes without a past history of ocular surgery, the mean central corneal thickness was 643.05 ┬▒ 37.67 ┬Ąm. In 27 eyes, the mean endothelial cell count was 3,349.44 ┬▒ 408.17 cells/mm2. The endothelial cell count could not be obtained in 8 eyes with significant corneal surface irregularities or corneal clouding.
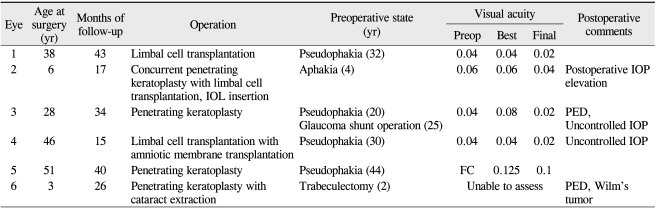
Ocular surface surgeries were performed in 6 eyes (10.0%) due to marked corneal clouding that affected VA. The surgical results are summarized in Table 4. Postoperative intraocular pressure (IOP) elevation occurred in 3 eyes and a persistent epithelial defect was a complication in 2 eyes. After surgery, the clarity of the transplanted corneal graft vanished with progression of peripheral neovascularization, subepithelial fibrosis, and thickening of the grafted cornea. Only one eye had an improvement in final VA.
Aniridic glaucoma
Glaucoma was found in 31 eyes (51.6%). Twelve eyes had newly detected glaucomatous optic disc changes and 17 eyes were already being treated with topical medication because the diagnosis of glaucoma had been made at another clinic.
Of the 14 eyes from the 7 patients under the age of 20, 10 eyes (71.4%) from 5 patients had glaucoma. One male and one female infant had congenital glaucoma in both eyes and both had undergone bilateral trabeculectomy. Four eyes from 2 patients were diagnosed with glaucoma during the early teen years. Two eyes were complicated with glaucoma after keratoplasty and cataract surgery, respectively.
Among the 46 eyes from 24 adult patients with an age greater than 20, 21 eyes (45.7%) of 11 patients had glaucoma.
Three eyes had undergone Ahmed valve implantation and 6 eyes had undergone trabeculectomy. Twenty-two eyes had glaucoma controlled with topical anti-glaucomatous medications.
Cataract
Twenty eyes had a prior history of cataract extraction. Their mean age at the time of cataract extraction was 25.75 years.
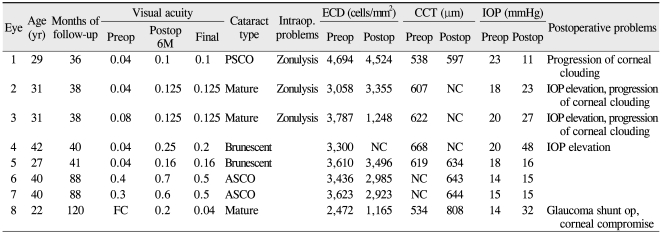
Of the remaining 40 eyes, lens opacity was found in 33 eyes (82.5%) at the initial visit. Five eyes exhibited lens subluxation combined with zonular weakness. Young patients had a mild degree of anterior or posterior subcapsular lens opacity, as shown in Fig. 1A. Table 5 summarizes the clinical features of 8 eyes in which phacoemulsification and implantation of an intraocular lens were performed. The mean age at the time of cataract surgery was 29.8 ┬▒ 5.9 years and the mean preoperative endothelial cell count was 3,497.50 ┬▒ 383.11 cells/mm2. At the time of cataract surgery, the mature and brunescent types of lens opacities predominated. Anterior vitrectomy with transscleral fixation of the intraocular lens was performed in 3 eyes with weak zonules. Postoperative 6-month VA improved in all of these eyes. Four eyes suffered from the development or deterioration of glaucoma. Corneal clouding and peripheral neovascularization became worse after cataract surgery in 4 eyes, one of which required corneal transplantation surgery.
Foveal hypoplasia
A fundus examination was possible in 44 eyes that were without significant corneal or lens opacity. Foveal hypoplasia, defined as the absence of a foveal reflex (Fig. 1B), was found in 36 eyes (81.8%).
Combined ocular and systemic anomalies
One male infant with a positive familial history for congenital aniridia had Peter's anomaly and congenital glaucoma in both eyes. One female infant with sporadic congenital aniridia was also diagnosed with congenital glaucoma. Wilm's tumors were found in two children (6.5%) with sporadic congenital aniridia. The Wilm's tumors were diagnosed at 40 and 33 months after birth, respectively; these 2 patients were treated with nephrectomy and chemotherapy.
Discussion
Approximately 30 cases of congenital aniridia have been reported in Korea since the first report of 4 cases of congenital aniridia in Koreans in 1977 [8-11]. Recently, Kim et al. [11] reported the presence of PAX6 gene mutations in 12 Korean aniridia patients. This study investigated Korean aniridic patients to estimate the prevalence and characteristics of associated disorders, disease course, and visual prognosis. In summary, cataract, keratopathy, and foveal hypoplasia were present in over 70% of the Korean patients with congenital aniridia. Glaucoma was present in about half of the patients. Very few of the aniridic patients had VAs better than 20/60. The primary factor in the progressive decrease in VA is thought to be deterioration of the associated keratopathy with aging. The majority of the patients in this study were in their twenties (38.7%) and thirties (25.8%), with the most common chief complaints including a progressive decrease in VA due to cataract and keratopathy and uncontrolled intraocular pressure.
It is well-established that aniridic keratopathy is the result of a limbal stem cell deficiency [4,12,13]. A peripheral pannus with a relatively clear central cornea was also observed in the majority of the young patients in this study. With age, neovascularization gradually advances into the central cornea until the entire cornea is involved. Subepithelial fibrosis and stromal haze were also observed. The central corneal thickness increased to 643.05 ┬▒ 37.67 ┬Ąm with a relatively normal endothelial cell count (3,349.44 ┬▒ 408.17 cells/mm2), which was comparable to other previously reported results [14,15]. A thickened cornea was presumed to be caused by developmental changes in the epithelium and stroma and not by endothelial dysfunction. In this study, more than half of the patients under the age of 20 years had worse than grade 1 keratopathy. Preservative-free lubricants and autologous serum eyedrops are helpful in patients with early stage keratopathy [13,16-18].
In this study, the long term surgical results of penetrating keratoplasty with or without limbal allograft were very poor. A persistent epithelial defect caused by a limbal cell deficiency and postoperative IOP elevation were common problems following keratoplasty. The same pre-graft corneal changes recurred and led to graft failure. All the eyes that had undergone keratoplasty had a prior history of cataract or glaucoma surgery. These patients had higher grade keratopathy in their pseudophakic or aphakic eyes compared to their phakic contralateral eyes. Aniridic keratopathy can worsen following surgery that involves excessive manipulation of the limbus [6].
Cataract was the most common associated disorder in the aniridic patients and increased with age. The mean age at the time of cataract surgery was 29.8 ┬▒ 5.9 years.
There was a relatively high risk of intraoperative and postoperative complications in these aniridic cataract patients. They exhibited fragile anterior lens capsules and associated lens subluxation or weak zonules. Deterioration of glaucoma was the main postoperative problem and was observed in 4 eyes (50%). In addition, we found that corneal clouding became worse after cataract surgery in 4 eyes (50%). This clouding was caused by edematous changes due to endothelial dysfunction in 1 eye or progressive stromal haze unrelated to endothelial dysfunction in 3 eyes. Aniridia has a profibrotic nature [16,19]. Reinhard et al. [20] found postoperative deterioration of corneal surface disorders in 4 eyes and chronic endothelial cell loss in 3 eyes among 19 congenital aniridic patients. The proximity of the intraocular lens to immature vessels in the rudimentary iris, subclinical chronic inflammation, and the unique vulnerability to progressive fibrosis caused by PAX6 gene mutations may be possible mechanisms for the observed progressive fibrosis following cataract surgery in eyes with congenital aniridia [19]. Progressive corneal clouding and glaucomatous changes can also impede final VA. Early cataract surgery is not advisable in aniridic patients; however, it was difficult to definitively determine the impact of this surgery on visual prognosis because of the small number of cases in this study.
The incidence of glaucoma in cases of congenital aniridia has been reported to range from 6% to 75% [18,21,22]. In this study, 51.6% of the patients had glaucoma. Glaucoma usually develops during late childhood in patients with congenital aniridia and is related to progressive circumferential changes in the angle, along with the gradual forward migration of abnormal iris tissue and the obscuration of the posterior trabecular meshwork and scleral spur [18,21]. In this study, the prevalence of glaucoma (71.4%) was also high in patients under the age of 20. In addition, congenital glaucoma was observed in 2 patients. Young patients with aniridia should be kept under close surveillance for the development of glaucoma. Increased central corneal thickness leads to a significant overestimation of the IOP in patients with congenital aniridia. Therefore, careful and regular examinations of the optic disc are very important for the detection and management of glaucoma in patients of all ages with congenital aniridia. Surgeons should also be aware that glaucoma can develop or deteriorate after cataract or corneal transplantation surgery.
Foveal hypoplasia may partially or entirely be responsible for visual impairment in patients with congenital aniridia. In previous reports, the incidence of foveal hypoplasia in cases of congenital aniridia has been reported to range from 50 to 74% [1,5,6]. Patients with congenital aniridia exhibit retinal dysfunction of varying degrees. This retinal dysfunction can be accounted for by foveal hypoplasia secondary to PAX6 mutation or phototoxicity as a result of a maldeveloped iris. Photophobia may be caused by macular hypoplasia, but not by a large pupil.
Wilm's tumors were found in two children with sporadic congenital aniridia. Because the PAX6 gene is in close proximity to the WT1 gene, deletions of 11p13 involving both the PAX6 and WT1 genes could result in the presence of a Wilm's tumor in addition to congenital aniridia [18]. Children with congenital sporadic aniridia develop Wilm's tumor before the age of 2 to 3 years. Ophthalmologists should be aware of this systemic association with malignancy, especially in sporadic cases. All children with sporadic aniridia should undergo repeated abdominal ultrasonography and clinical examinations.
In conclusion, congenital aniridia is a progressive congenital disorder that is commonly accompanied by complications that can lead to impaired vision, including cataract, keratopathy, glaucoma, and foveal hypoplasia. The long-term surgical results of penetrating keratoplasty with or without limbal allograft were very poor in this study. There was also a high risk of intraoperative and postoperative complications in aniridic cataract patients. Progressive corneal clouding or glaucomatous damage can impede final VA following cataract surgery. Regular and careful examinations for accompanying complications are necessary in all patients who suffer from congenital aniridia.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






