

Silicone oil used in vitreous retinal surgery may cause the deterioration of visual acuity by adhering to silicone intraocular lenses. Further, when this adhesion develops, not only does it render subsequent surgery difficult, it may also necessitate removal or exchange of the intraocular lenses.
Here we report the case of a female patient with a history of silicone oil removal surgery where the resulting silicone bubbles had not been removed thoroughly and remained in the vitreous cavity. These bubbles subsequently adhered to the intraocular lens following YAG laser posterior capsulotomy, resulting in refractive changes.
Case Report
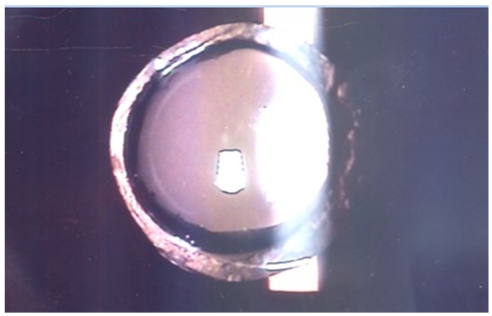
A 32-year-old female patient underwent vitrectomy, air-fluid exchange, and silicone oil injection in the left eye for the treatment of proliferative diabetic retinopathy in October 2002. Six months after the ambulatory follow-up, vitrectomy, air-fluid exchange, and silicone oil injection were performed on her right eye for the treatment of proliferative diabetic retinopathy. Silicone oil removal surgery was performed on the left eye. In January 2004, silicone oil removal surgery was performed on the right eye. In February 2004, per the manifest refractive test, the right eye was -sph1.25 and the left eye was +sph1.00; the best corrected visual acuities were 0.3 and 0.2, respectively. During the ambulatory follow-up, together with deterioration of the left eye visual acuity, the progression of a severe cataract was detected, and thus cataract surgery was recommended. In June 2004, the patient visited our hospital again for acute vision deterioration. Through an examination of the patient history we found that, in April 2004, in a private clinic, extra-capsular cataract extraction by phacoemulsification and intraocular lens insertion (Silicone, LI61U; Bausch & Lomb, Rochester, NY, USA) were performed on her left eye, and in May 2004, YAG laser posterior capsulotomy was performed. By slit lamp examination, adhesion of silicone oil bubbles to the posterior side of the intraocular lens through the posterior capsulotomy window was observed (Figs. 1 and 2). The result of manifest refraction testing was -sph16.00=-cyl0.50 Ax 90┬░, and the best-corrected vision was measured as 0.4.
In July 2004, intraocular lens (Acryl, Akreos adapt; Bausch & Lomb) exchange surgery was performed. Due to the adhesion of the silicone oil, the visual acuity of the intraocular lens could not be calculated accurately, and thus an intraocular lens with an A constant and a diopter identical to the previous lens was used to replace the contaminated lens. In manifest refractive testing performed in May 2005, the left eye was -sph1.25=-cyl0.50 Ax 90┬░, and the best corrected visual acuity was 0.4.
Discussion
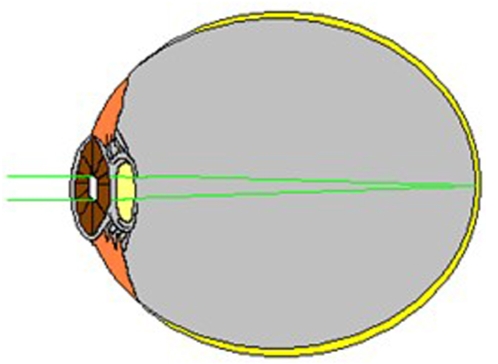
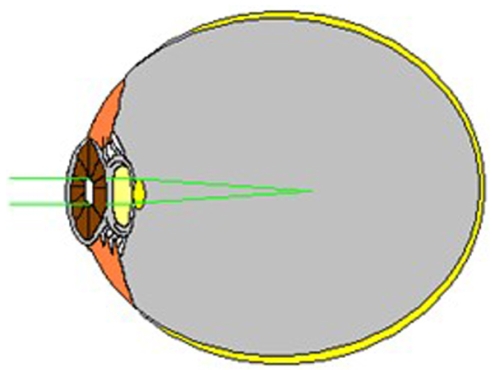
Generally, silicone oil injected into the vitreous cavity induces hyperopic deviation.1,2 This is due to the fact that the refractive index of silicone oil (RI=1.405) is higher than that of the vitreous body or the aqueous fluid (RI=1.336). In 2005, Hotta and Sugitani3 reported a change of refractive power in the pseudophakic eye injected with silicone oil. They reported that with injected silicone oil into the vitreous cavity, an average +5.69┬▒1.71 diopters of hyperopic deviation of spherical aberration was found. Conversely, after the removal of silicone oil, -5.63┬▒1.33 diopters of spherical aberration change was found. In the current case, in manifest refraction testing performed prior to and after surgery, +14.75 diopters of spherical aberration change was observed. It is believed that the reason for the development of such a large change in refractive power is the accumulation of silicone oil in the narrow posterior sac incision window acting like a convex lens (Figs. 3 and 4).
The adhesion of silicone oil to an intraocular lens occurs frequently when the material of the optic zone is silicone.4-7 In the present case, adhesion of silicone oil to the intraocular lens where the optical area was silicone was observed.
The adhesion of silicone oil to an intraocular lens is irreversible in most cases. Apple et al.8 reported three cases that demonstrated irreversible adhesion of silicone oil to silicone intraocular lenses. They found that in these three cases, the silicone oil could not be removed by mechanical force or through the injection of viscoelastic materials.
As it is difficult to remove silicone oil adhered to intraocular lenses, the removal or exchange of the lens may be required. Therefore, preventing the adhesion of silicone oil to intraocular lenses is critical. We believe the insertion of a silicone intraocular lens should be avoided in patients who may use silicone oil in the future or who underwent previous silicone oil removal surgery. Also, when performing a posterior capsulotomy in a pseudophakic eye without knowing the particulars of the patient's past ocular history, one should consider the possibility of the adhesion of silicone oil to an intraocular lens; again demonstrating the critical importance of an accurate history in medicine.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






