

Vogt-Koyanagi-Harada disease (VKH) is a systemic autoimmune disorder affecting pigmented tissues in the ocular, auditory, integumentary and central nervous systems.1 Graves' disease is an immune disorder, most commonly caused by hyperthyroidism. Previously, a case of VKH that developed in a patient with Hashimoto's thyroiditis was reported.2 However, the explanation for the association of hyperthyroidism and VKH remains unclear. Here, we describe a case of VKH that developed in a patient with Graves' disease.
Case Report
A 36-year-old woman was referred for blurred vision in both eyes that had lasted for three days. She complained of a stiff neck and headache occurring over the same period. She had been diagnosed with Graves' disease one year previously and was treated with methimazole. However, she had discontinued the methimazole seven months prior, because she was diagnosed with methimazole-induced hypersensitivity following development of a skin rash. After discontinuing the methimazole, the patient was treated with Lugol's solution with 30 mg of prednisolone. After three months, she complained of lower limb weakness. A muscle biopsy was performed, revealing prednisolone-induced myopathy. The dose of prednisolone was reduced to 10 mg. After symptoms developed, she was taken to the hospital for evaluation of systemic diseases in the allergy division of the Department of Internal Medicine. She was referred to retinal clinic for ocular examination.
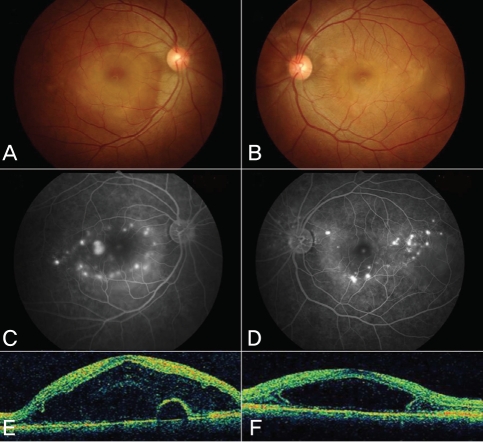
On examination, her best-corrected visual acuities (BCVA) were 20/100 in both eyes. The anterior chamber was within normal limits. A fundus examination showed disc edema accompanied by a serous retinal detachment in both eyes (Fig. 1 A and B). Fluorescein angiography (FAG) showed multiple leaks at the posterior pole (Fig. 1 C and D). In addition, optical coherence tomography (OCT) revealed subretinal fluid (Fig. 1 E and F). Initially, we suspected prednisolone-induced central serous chorioretinopathy. We decided to observe the patient closely with predisolone tapering to 5 mg for 1 week.
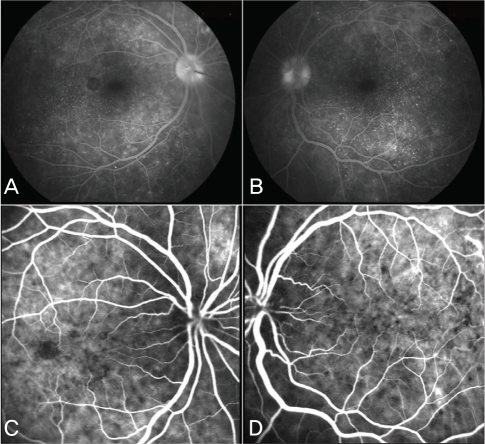
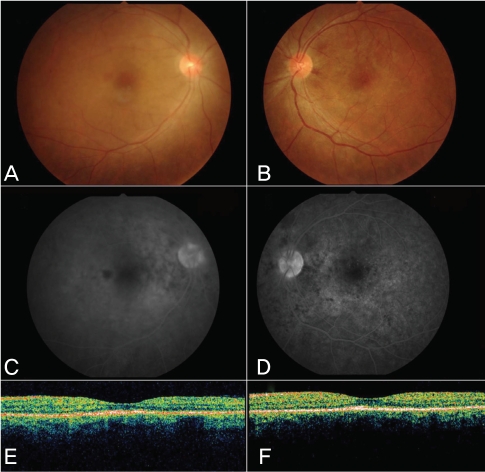
After seven days, the patient's visual acuity did not change, but the subretinal fluid buildup and the retinal detachment worsened. Simultaneously, anterior chamber reaction and vitreous haze developed in both eyes. The leakage pattern on FAG changed (Fig. 2 A and B), and indocyanine green angiography revealed multiple hypofluorescent spots (Fig. 2 C and D). A lumbar puncture revealed pleocytosis with 21 mononuclear cells/dL. The patient was diagnosed with VKH disease and treatment with high dose steroid pulse therapy was recommended. Although the internal medicine physicians were reluctant to use steroids due to the patient's steroid-induced myopathy, intravenous administration of 500 mg of methylprednisolone for three days followed by 30 mg prednisolone with 75 mg of cyclosporine per day was provided. After 40 days, her BCVA recovered to 20/40 OD, 20/25 OS. Fundus examination showed attached retinas bilaterally, and FAG revealed that the leaks had resolved in both eyes (Fig. 3).
Discussion
Since both VKH and Graves' disease are caused by T cell-mediated autoimmune dysfunction, they might share a common pathogenic process.3,4 Moreover, in this case, altered immune regulation that may have resulted from drug-induced hypersensitivity may have contributed to the development of VKH. Although our patient received 10 mg of prednisolone, this did not prevent the development of VKH. This case study illustrates the diagnostic and therapeutic challenges of VKH-associated autoimmune diseases.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






