

Canalicular laceration is the most common type of trauma to the lacrimal system. In order to prevent posttraumatic epiphora, lacerated tear ducts should be repaired quickly and accurately. In addition, meticulous wound approximation of the canaliculus is critical for reestablishing the patency of the damaged system; and any technique utilized should be atraumatic to adjacent uninjured parts of the nasolacrimal anatomy.
When the laceration occurs to the canaliculus of the lacrimal system, both medial and lateral cut ends of the tear ducts are retracted due to its elasticity. If the laceration is close to the punctum, the medial canaliculus will be near the lid margin and a repair may be relatively simple. However, if a traumatic laceration occurs close to the lacrimal sac, the common canaliculus will be retracted deep into the medial canthal tendon and surrounding tissues. In this type of injury, the surgeon must look deeper for the medial canaliculus; and it can be very tedious to localize the medial cut end, which lies in deep tissues. For this reason, various techniques to localize the lacerated cut end have been reported.1-9 However, these procedures are regarded as complicated operative procedures with a higher degree of difficulty; and because of this, postoperative complications such as epiphora tend to increase.
Our authors experienced lower canalicular lacerations resulting from trauma, and utilized lacrimal probing through the uninjured upper canaliculus to locate the proximal cut end of the lacerated canaliculus on reconstruction. This procedure proved to be the most useful method compared to those in previous studies, in the sense that it utilizes the least time and causes minimal damage.
Herein, we report the simple procedure of lacrimal probing through the uninjured upper canaliculus as an effective method of locating the proximal cut end of the lower canalicular laceration.
Materials and Methods
From September 2003 to December 2006, 27 patients with canalicular laceration visited the Konyang University Hospital. All cases were repaired by one surgeon, who utilized lacrimal probing on lower canalicular reconstruction to locate the lacerated medial cut end. The total operative time necessary to identify the cut end was measured, and the usefulness of probing was evaluated.
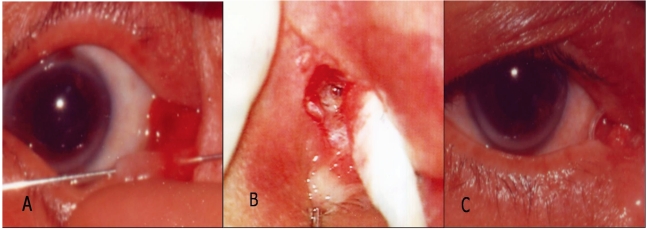
Patients with injuries in the medial canthus due to trauma were examined by lacrimal probing and saline irrigation. If the patient had a lower canalicular laceration, surgery was performed within 48 hours after the injury, and identification of the cut end was attempted under an operating microscope. (Fig. 1A) When the laceration occurred medially, identifying the medial end of the canaliculus was difficult despite adequate magnification, and lacrimal probing with a Bowman probe was performed through the dilated upper punctum. The probe passes from the uninjured punctum to the inferior meatus in the nasal cavity through the nasolacrimal duct. By manipulating the lacrimal probe placed in the intact canaliculus, the lacrimal sac and the common canaliculus can be pushed towards the operative field, thus improving visualization of the canalicular cut end. (Fig. 1B) This procedure helps the surgeon locate the injured canaliculus by palpation with a cotton ball. The surgeon was then able to identify either the lacerated canalicular proximal end, which has rolled white edges and a shiny epithelial lining, or the metal surface of the probe through the canalicular lumen. Demonstrating the lumen of the cut end, a Crawford silicone tube was intubated through the exposed cut medial end, while the lacrimal probe was simultaneously removed. The other end of the Crawford silicone tube was intubated through the ipsilateral uninjured upper punctum and retrieved from the nose. The lacerated pericanalicular tissue and medial canthal tendon was then repaired with 5-0 and 6-0 vicryl sutures. The lid margin and skin are closed with a typical marginal lidlaceration repairing method, using 6-0 nylon or 7-0 black silk, and the silicone is tied in a tight square knot.
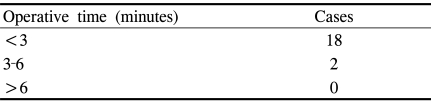
The authors measured the total time necessary to identify the medial cut end. The silicone tube was maintained for approximately 6 months (Fig. 1C), and 0.3% ofloxacin and 0.1% fluorometholone eyedrops were used postoperatively. Postoperative results were judged by subject symptoms and tearing in the follow-up period.
Results
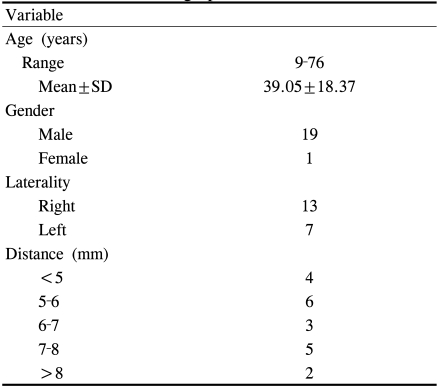
A total of 27 cases with lower canalicular lacerations due to trauma were involved in this study; and canalicular reconstruction was performed within 48 hours after injury in all patients. Twenty-seven eyes with lower canalicular lacerations were reconstructed under a microscope. Seven out of 27 eyes had superficial injuries, with a mean distance of 2.3 mm from lacrimal punctum to the medial cut end. We were able to identify the medial cut end in these eyes without any difficulty under a microscope; however, in the other 20 cases it was difficult to find the cut end, because the lacerated sites were relatively deep. In these cases, an upper canalicular probing technique was used to identify the medial cut end of the lacerated lower canaliculi. Table 1 displays the distances of their lacerated sites. The mean distance was 6.1┬▒1.8 mm from the lacrimal punctum to the medial lacerated end. Approximately, 2.0┬▒1.1 minutes were utilized to identify the cut end on average (Table 2). If the medial cut end of the lacerated canaliculus was identified, a silicone tube was intubated between the medial cut end and the lateral cut end. Average patient follow-up time post-operatively was eight months, and the average time to extubation was 4.8 months (Table 3). None of the patients reported lacrimation, and all of the patents had a patent nasolacrimal apparatus on final follow-up.
Discussion
The fundamental principle in repairing a lacerated canaliculi is to establish patency of the damaged lacrimal system. Quick and accurate repair of the lacerated tear ducts with minimal iatrogenic trauma provides much better functional results. However, the most difficult part of surgical repair may be identifying the damaged medial cut end of the canaliculus. Many techniques, such as pig tail probing, the air bubble test, injection of colored opaque or viscous solutions, and sympathominetics drugs have been utilized to identify the medial cut end. However, these tests are not without their drawbacks. Pig tail probing could have a high incidence of failure, potential false passages, or possible damage to the uninjured portion of the system.1,3-6 The air bubble test requires a closed system,1,2,7-9 and the use of colored solutions may make the operative field obscure.1,2 Nevertheless, although various methods have been discussed, many surgeons continue to encounter difficulty in finding the lacerated medial cut end.
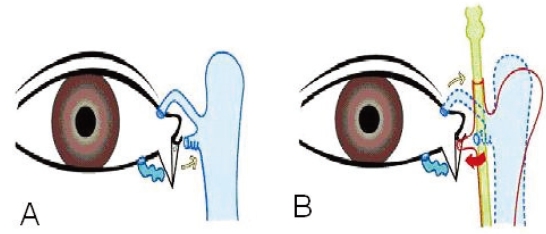
The authors attempted lacrimal probing from the uninjured upper canaliculus to the nasolacrimal duct to determine the location and the direction of the lacrimal sac. This made it possible to identify the laterally lifted lacrimal sac and the lacerated canalicular opening via palpation of the probe using a cotton ball. The lacerated medial end was found with rolled white edges and a shiny epithelial lining. Thus, lacrimal probing through the uninjured upper canaliculus improved identification of the lacrimal sac and common canaliculus. These structures could then be moved laterally for straightforward exposure. (Fig. 2) The authors were then able to find the lacerated proximal end more quickly and easily.
When attempting to perform probing through the damaged canaliculi, a false passage may be formed, increasing the difficulty of the operative procedures. In this case, probing via the undamaged canaliculi through the inferior meatus opening may reduce false passage formation.
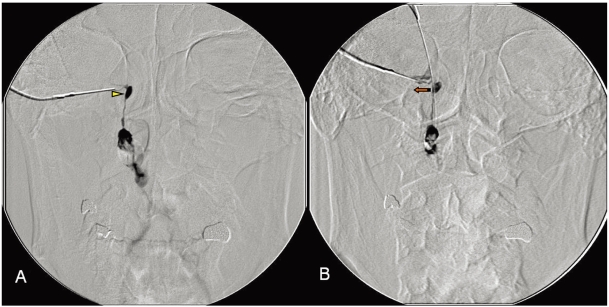
We confirmed the effect of lacrimal probing by means of dacryocystography (DCG) with lacrimal probing on normal anatomy. The DCG provided a view of the lateralized lacrimal sac after probing (Fig. 3).
After locating the lacerated canalicular tip, a bicanalicular silicone tube was inserted. We did not use monocular stents, although they may minimize the risk of injury to the intact canaliculus, because they have a high potential for retention. We preferred that a silicone tube be passed through both canaliculi and down the nasolacrimal duct. This type of stent is both well-tolerated and effective.9
After inserting the stent, pericanalicular tissue suture was performed. Direct suturing of the canaliculus is unnecessary, provided that a stent is placed and the surrounding tissues are approximated.9 Robert C. Kersten et al. reported a retrospective study involving 67 patients, and concluded that simple re-approximation of the lacerated overlying soft tissue combined with bicanalicular silicone intubation is a highly successful procedure for managing canalicular lacerations. In their report, they explain that the indwelling silicone tube keeps the canalicular edges adequately approximated, eliminating the need for canalicular suturing.10
Lacrimal probing, a basic procedure utilized for identifying the patency of the nasolacrimal duct, results in less iatrogenic trauma. It was especially useful in deeper lower canalicular lacerations, i.e., those that were 7 mm or more apart from the punctum. The average time utilized to find the lacerated end using the lacrimal probing procedure was 2 minutes; however, in some cases, we were able to identify the cut end in less than one minute, even in cases in which the wound was considerably deep. To this author's knowledge, our method was the easiest and quickest technique for locating the medial cut end of a lacerated canaliculus. The lacrimal probing method could save operative time and improve success rates significantly in repairing canalicular damage. Consequently, our technique makes canalicular reconstruction a considerably easy procedure.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






