

A variety of different types of pigment epithelium
detachment (PED) have been identified in the medical
literature. These types of PED can be classified as
fibrovascular PED, serous detachment of RPE, hemorrhagic
detachment of RPE and drusenoid RPE detachment.1
Verteporfin photodynamic therapy (PDT) has been used to
safely reduce the risk of loss of vision in patients with
choroidal neovascularization (CNV) in age-related macular
degeneration.2 We performed PDT on a patient with drusenoid
PED and here report the clinical course.
Case Report
A 68-year-old man presented with decreased visual acuity
in his left eye for several months. His corrected vision in the
left eye was 20/40. There was no abnormality observed in
the anterior segment. On fundus examination of the left eye,
one disk diameter sized PED, with diffuse coalesced soft
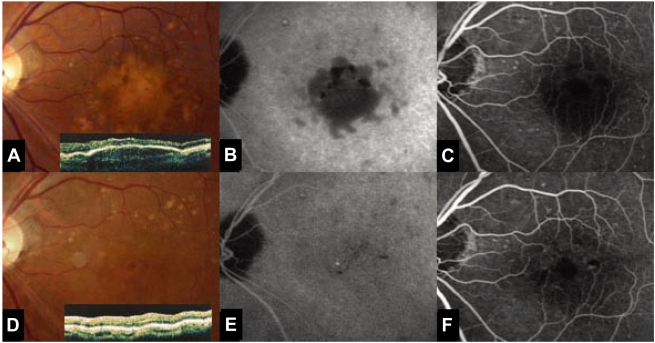
drusen was noted at the macula. At the first examination,
fluorescein angiography revealed delayed, regular hyperfluorescence
without leakage and the OCT showed multiple
pigment epithelium detachments. There was no evidence of
CNV (Fig. 1A, B, C). PDT was performed at the PED site
and around 1,000 ┬Ąm2. Fifteen days after PDT, the corrected
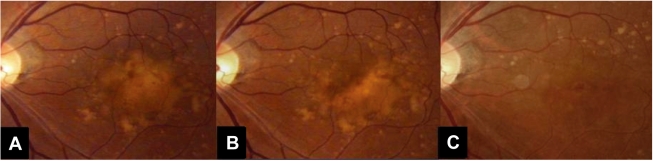
vision for the left eye was 20/40. On the fundus examination,
there was no interval change (Fig. 2A). Five months after
PDT, the fundus examination showed a decreased size of the
soft drusen (Fig. 2B). Ten months after PDT, the corrected
vision of the left eye was improved to 20/25. On fundus
examination and OCT, the number of soft drusen was
markedly decreased (Fig. 2C). ICG showed that the drusenoid
PED diminished in size (Fig. 1D, E, F).
Discussion
Drusenoid PED has been distinguished from other types of
injury by its better prognosis. This avascular PED typically
develops slowly and causes minimal complaints of blurred
vision. The natural history usually follows a progression to
persistent drusenoid RPE detachment, geographic atrophy and
neovascularisation.3 The effect of PDT on drusenoid PED has
not been confirmed, but the effect of a grid laser on drusen
has been reported.4
The effects of PDT can be divided into the photochemical
effect of verteporfin and the effect of the 689 nm nonthermal
laser itself. As previously reported, vertiporfin has a very
broad absorption spectrum, but only the far-red peak at
688-691 nm is typically used in clinical practice. A beam of
red laser light (689 nm diode laser) is applied to the retina
via a slit lamp irradiating a spot of about 1 mm in diameter,
with light intensity of 600 mW/cm2, for 83 seconds, resulting
in a total radiant exposure of 50 J/ cm.2,5 Closure of abnormal
(leaking) blood vessels occurs for approximately 6-12 weeks
in most patients.
We suspect that direct laser treatment of drusen may
accelerate their removal by phagocytes, and that RPE
proliferation induced by laser photocoagulation might reduce
the amount of debris per cell and enhance the phagocytic
capacity of the RPE.6 Indirect effects of the laser may alter
the characteristics of the lipids which cause Bruch's
membrane impairment, so that the soft drusen material
escapes.7
In our case, PDT was effective for reducing the drusenoid
PED. The effect was observed ten months after the PDT we
thought the effect was caused by the laser, not the
verteporfin. The efficacy of 689 nm diode laser on drusenoid
PED has not been reported; the long term efficacy of the
conventional PDT treatment is not known. Further studies are
therefore warranted.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






