Endogenous Aeromonas Hydrophila Endophthalmitis in an Immunocompromised Patient
Article information
Abstract
Purpose
To report a case of endogenous endophthalmitis due to Aeromonas hydrophila in a patient with distal common bile duct carcinoma and biliary sepsis.
Methods
A 72-year-old woman with distal common bile duct carcinoma, obstructive jaundice, diabetes mellitus, and hypertension had a 1-day history of blurred vision, redness, and eye discharges in the right eye. An ophthalmic examination showed no light perception vision, increased intraocular pressure, severe corneal edema, severe anterior chamber reaction, exudative membranes on the anterior lens surface, and severe vitreal reaction. There was no ocular history of trauma, infection, or surgery in either eye.
Results
Under the impression of endogenous bacterial endophthalmitis, immediate intraocular cultures and intravitreal antibiotic injections were performed, but the anterior chamber reaction, and the ultrasonogram findings were deteriorated. Evisceration was undertakened because of extrusion of the intraocular contents, and Aeromonas hydrophila was isolated by intraocular culture.
Conclusions
Endogenous endophthalmitis due to Aeromonas hydrophila is rare, but has a rapid clinical course and a poor prognosis, despite of prompt diagnosis and management.
The genus Aeromonas consists of gram-negative, facultatively anaerobic, rod-shaped, oxidase-positive bacteria that are widely distributed in the aquatic environment. In humans Aeromonas hydrophila may cause traumatic wound infection, gastroenteritis, and septicemia, especially in immunocompromised hosts, but endogenous endophthalmitis caused by this agent is rare. Two reports of endogenous endophthalmitis have been described in immunocompetent patients.1,2 However, to the best of our knowledge, this is the first case of endogenous endophthalmitis caused by Aeromonas hydrophila in an immunocompromised patient.
Case report
A 72-year-old woman with distal common bile duct carcinoma, obstructive jaundice, diabetes mellitus, and hypertension was admitted to our gastroenterology department. Two days after admission, ophthalmic consultation was sought to evaluate diabetic retinopathy. At initial examination, best-corrected visual acuity was 20/50 in both eyes with incipient cataract, but no sign of diabetic retinopathy. Moreover, there was no ocular history of trauma, infection, or surgery in either eye. Three days later, on day 5 after admission, the patient reported a 1-day history of blurred vision, redness, and eye discharge in the right eye. The patient was alert enough to have promptly reported her symptoms. Ophthalmic examination of the right eye showed a best-corrected visual acuity of no light perception, severe chemosis and injection of conjunctiva, and corneal haziness. Slit-lamp examination revealed an increased intraocular pressure of 30 mmHg, severe corneal edema, a shallow anterior chamber, severe anterior chamber reaction (many cells, flare, and RBCs), exudative membranes on the anterior lens surface, and a mid-dilated pupil (Fig. 1A). Fundus examination was obscured by severe vitreal reaction. A B-scan ultrasonogram showed moderate vitreous opacities (Fig. 1B). Ophthalmic examination of the left eye was unremarkable. Under the impression of endogenous bacterial endophthalmitis, immediate intraocular cultures (anterior chamber paracentesis 0.2 ml, vitreous needle aspiration 0.3 ml) and intravitreal antibiotic injections (vancomycin 1 mg/0.1 ml, ceftazidime 2 mg/0.1 ml) were performed with subsequent intravenous antibiotic therapy (Meropenem 2 g per day). Because of corneal haziness, it was impossible to treat the endophthalmitis surgically. Despite the intravitreal injections the anterior chamber reaction and ultrasonogram findings deteriorated, with inferior protrusion of the globe (Fig. 2). Intraocular Gram staining revealed 2+ gram-negative rods and 4+ Aeromonas hydrophila sensitive to ceftazidime by intraocular culture. Culture results from urine and bile juice were positive for Acinobacter Iwoffi/baumannii and Enterobacter aerogenes, respectively. However, blood culture results were negative for Aeromonas hydrophila. On day 8 after admission, percutaneous transhepatic biliary drainage was done to control total bilirubin, and on day 6 after intravitreal injections, limbus perforation occurred with extrusion of the intraocular contents (Fig. 3). Evisceration and Medpor® (porous polyethylene, Porex Surgical, College Park, GA, U.S.A.) sphere implantation was done. On day 40 after admission, the patient was discharged from hospital with controlled jaundice, when her predicted survival was less than one year.

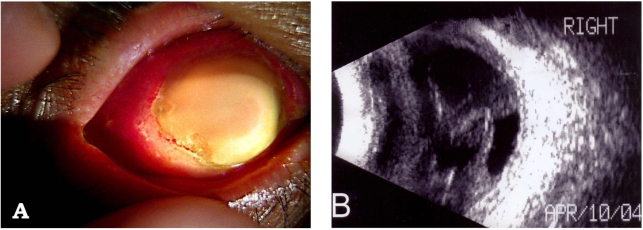
A. Slit-lamp photograph at initial presentation: Severe corneal edema, hyphema, exudative membranes on anterior lens surface, and mid-dilated pupil.
B. B-scan ultrasonograph at initial presentation: Moderate vitreous opacities.
A. Slit-lamp photograph on the day 2 after intravitreal injections: Totally opaque cornea and inferior protrusion of the eyeball.
B. B-scan ultrasonograph on the day 2 after intravitreal injections: Increased and condensed vitreous opacities.

A. Slit-lamp photograph on the day 6 after intravitreal injections: Perforation of the eyeball.
B. Computed tomograph on the day 6 after intravitreal injections: Contracted right eyeball with internal increased densities.
Discussion
Endogenous bacterial endophthalmitis is a rare but potentially sight-threatening condition that occurs when organisms reach the eye via the bloodstream and cross the blood-ocular barrier. It accounts for only 2-6% of all cases of endophthalmitis.3 Because prompt management is mandatory for saving the eye, clinicians must have a high index of suspicion of this rare but serious condition.
Aeromonas species are important pathogens of fish and a variety of animals, and can be pathogenic in patients infected by a contaminated wound or in the immunocompromised. Aeromanas hydrophila has been reported to cause endophthalmitis after a penetrating injury,4 post-traumatic keratitis,5 contact lens-related keratitis,6 and endogenous endophthalmitis.1,2
The presence of many RBCs in the anterior chamber is not typical of endophthalmitis, and has not been found in other reported cases of Aeromonas hydrophila.1,2 However, in the present case we found hyphema. Although our patient was not overtly immunocompromised, risk factors such as old age, diabetes, hypertension, and malignancy may have predisposed a state of immune dysfunction. The patient had distal common bile duct carcinoma with obstructive jaundice, but the exact source of the infecting organism remains unclear. It is possible that Aeromonas hydrophila was contracted from a long indwelling catheter rather than direct spread from biliary sepsis. In common with two previous reports,1,2 this case also showed a rapidly worsening course and a poor prognosis despite prompt diagnosis and management.