Investigation of the Association between Normal-tension Glaucoma and Single Nucleotide Polymorphisms in Natriuretic Peptide Gene
Article information
Abstract
Purpose
The expression of natriuretic peptides in the neural bundles of the anterior portion of the optic nerves and their functions in regulating vessel tone and blood flow may suggest a possible role in the pathogenesis of glaucoma. The purpose of this study was to investigate the association between normal-tension glaucoma and the genetic variations of atrial natriuretic peptide (Nppa) and natriuretic peptide receptor A (Npr1) gene.
Methods
Sixty-seven Korean normal-tension glaucoma (NTG) patients and 100 healthy subjects (as normal controls) were enrolled. DNA from peripheral blood leukocytes was extracted, and the genotypes of five polymorphisms (c.94G>A, c.454T>C, IVS1+16C>T, IVS2+701G>A, and c.-764C>G) in the Nppa gene and one polymorphism (c.1023G>C) in the Npr1 gene were determined using the restriction fragment length polymorphism and the SNaPshot methods. The genotype and allele frequencies of these polymorphisms in patients with NTG and normal controls were compared using the Fisher's exact test and the chi-square test.
Results
In both groups, the genotype distributions were in accordance with the Hardy-Weinberg equilibrium. There was no significant difference in the frequency of the Nppa and Npr1 alleles or genotypes in the normal-tension glaucoma group as compared to the control group.
Conclusions
Nppa and Npr1 gene polymorphisms are not associated with normal-tension glaucoma, suggesting that this gene does not have an important role in the pathogenesis of optic neuropathy in this disease.
Glaucoma is a degenerative optic neuropathy characterized by optic nerve head changes and visual field loss, often related to raised intraocular pressure (IOP). Factors other than IOP are likely to have a role in the pathogenesis of glaucomatous optic neuropathy, particularly in individuals with normal-tension glaucoma (NTG). NTG is an entity of progressive glaucomatous optic neuropathy and corresponding visual field defects with IOP in the statistically normal range. Because of the normal IOP, other factors such as vascular dysregulation are supposed to play an important role in the pathogenesis of NTG. Since up to 21% of NTG patients were reported to have a family history, it is suggested that these patients may be genetically predisposed to developing NTG.1
The natriuretic peptide (NP) family is composed of atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP), and C-type natriuretic peptide (CNP).2-4 ANP and BNP are circulating peptides mainly produced in the heart that are involved in the regulation of natriuresis, diuresis, and blood flow.3,5 CNP predominantly acts as a vasodilator and is found principally in the central nervous system and endothelial cells.4,6 Three mammalian members of the natriuretic peptide gene family have been identified: Nppa, Nppb, and Nppc, which encode ANP, BNP, and CNP, respectively. The Nppa gene is located in 1p36.2 and contains three exons (Fig. 1A).

Genomic structures. (A) Nppa gene; (B) Npr1 gene (provided in the public domain by the National Center for Biotechnology Information, Bethesda, MD, U. S. A.; available at http://www.ncbi.nlm.nih.gov).
Three NP receptors -natriuretic peptide receptor A (NPRA), natriuretic peptide receptor B (NPRB) and natriuretic peptide receptor C (NPRC)- have been identified in mammalian tissue. NPRA and NPRB are linked to the cGMP-dependent signaling cascade and mediate many of the cardiovascular and renal effects of NPs. NPRA is activated by ANP and, to a lesser extent, BNP. NPRC plays a role in the clearance of the peptides, and it has been reported that NPs act to inhibit cardiomyocytes, vascular endothelial cells, and/or astrocyte proliferation in part through this receptor.7-10 The chromosomal locations of the genes encoding these three receptor subtypes are designated as Npr1, Npr2, and Npr3, corresponding to NPRA, NPRB, and NPRC, respectively. The primary structure of the Npr1 gene is located on 1q21-q22 and contains 22 exons interrupted by 21 introns (Fig. 1B).
NPs have been shown to inhibit vascular cell growth and regulate vessel tone, and may play an important modulatory role in angiogenesis.9,11 Rollin et al12 reported the expression of NPs in neural retinal, glial, and vascular elements in the normal adult retina, and also in the neural bundles of the anterior portion of optic nerves. This may present a role for these peptides in maintaining both the neural and vascular integrity of the mature retina and optic nerve. Collectively, these results may suggest that the NP system might be involved in the development of glaucoma.
In this study, we investigated the association between NTG and the single nucleotide polymorphisms in atrial natriuretic peptide and natriuretic peptide receptor A genes.
Materials and Methods
Subjects
The study population consisted of 67 patients with NTG and 100 healthy volunteers. All subjects were of Korean heritage and were apparently unrelated. NTG patients were recruited from the Glaucoma Clinic and volunteers from the Health Promotion Clinic of Seoul National University Hospital. Human subject participation and receipt of informed consent from each subject were approved by the Institutional Review Board of Seoul National University Hospital Clinical Research Institute.
The diagnostic criteria for NTG included normal intraocular pressure (IOP), glaucomatous optic disc cupping, glaucomatous visual field defects, an open anterior chamber angle, and the absence of any contributing ocular or systemic disorders. IOP was measured using a Goldmann applanation tonometer. Normal IOP was defined as a diurnal IOP persistently below 21 mmHg without medication. Visual fields of NTG patients were evaluated using the 30-2 program of the Humphrey Visual Field Analyzer Model 750 (Zeiss Inc., San Leandro, CA, U. S. A.) or Model 630 (Allergan Inc., San Leandro, CA, U. S. A.). Reliable fields were those with a fixation loss rate of ≤20% and false-positive and false-negative error rates of ≤20%. A glaucomatous visual field defect was defined as a Glaucoma Hemifield test outside normal limits on at least two fields, or a cluster of three or more non-edge points in a location typical for glaucoma (all of which are depressed on the pattern deviation plot at a P < 5% level, and one of which is depressed at a P < 1% level on two consecutive fields), or a corrected pattern standard deviation that occurs in less than 5% of normal fields.
Healthy volunteers who had completed medical and ophthalmological examinations at the Health Promotion Clinic served as controls. They had best corrected visual acuity of 20/25 and IOP of 21 mmHg or less. Subjects with any suspicious findings of glaucoma in the disc and fundus (e.g., cup:disc ratio of more than 0.6, notch in the neural rim, vertically oval cup, zone beta peripapillary atrophy, retinal nerve fiber layer defect, choroidal sclerosis, or abnormalities of the disc vessels) were not included. The two groups were compared with respect to average age, gender ratio, and IOP.
Gene polymorphisms
Six polymorphisms were identified through the review of articles. The exon 1 (c.94G>A), the exon 3 (c.454T>C), the intron 1 (IVS1+16C>T), the intron 2 (IVS2+701G>A) and the promoter region (c.-764C>G) polymorphisms in the Nppa gene, and the exon 3 (c.1023G>C) polymorphism in the Npr1 gene were selected and analyzed. Gene symbols and sequence variations are described according to the recommendations of the HUGO Gene Nomenclature Committee.13 The Nppa and Npr1 reference sequences are NCBI accession no. NC_000001.9 (http://www.ncbi.nlm.nih.gov; provided in the public domain by the National Center for Biotechnology Information, Bethesda, MD, U. S. A.).
The c.94G>A polymorphism was analyzed using the SNaPshot technique, and others were identified using restriction fragment length polymorphism with polymerase chain reaction (PCR). The primers used in this study are demonstrated in Table 1.
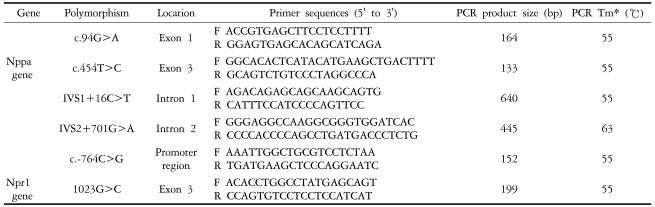
Primer sequences, polymerase chain reaction (PCR) product sizes, and PCR annealing temperatures
Genetic Analysis and Genotype Identification: PCR-RFLP reaction
Peripheral blood samples of NTG patients and controls were collected from the antecubital vein and stored in an EDTA tube for less than one day. Genomic DNA extraction was performed using a Gentra PureGene DNA isolation kit (Gentra System Inc., Minneapolis, MN, U. S. A.). PCR of the extracted DNA samples was performed on a final volume of 20 µL, which contained 50 ng of genomic DNA, 10 mM Tris-HCl (pH 8.3), 50 mM KCl, 1.5 mM MgCl2, 0.01% gelatin, 200 µM of each dNTP, 8 pmole of each primer and 0.5 U of Taq polymerase (AmpliTaq Gold™, Applied Biosystems, Foster City, CA, U. S. A.). The PCR conditions used were 95℃ for the initial 10 minutes, and 35 cycles of 95℃ for 30 seconds, each annealing temperature (Tm) for 30 seconds and 72℃ for 1 minute, and a final extension at 72℃ for 7 minutes. The annealing temperature of each primer for the PCR reaction is demonstrated in Table 1.
The PCR products obtained were then digested with restriction enzymes: ScaI for c.454T>C digestion yielded 77 and 56 bp fragments for the T allele and a 133 bp fragment for the C allele; BsxXI for IVS1+16C>T digestion yielded 442 and 198 bp fragments for the C allele and 262, 198, and 180 bp fragments for the T allele. MspI for IVS2+701G>A yielded 278, 136, and 31 bp fragments for the G allele and 309 and 136 bp fragments for the A allele, and BslI for c.-764C>G digestion yielded a 152 bp fragment for the C allele and 110 and 42 bp fragments for the G allele. TaqI for c.1023G>C of Npr1 gene yielded a 199 bp fragment for the G allele and 166 and 33 bp fragments for the C allele. The genotypes were identified after electrophoresis of the final digestion product in 2% agarose gel.
Genetic Analysis and Genotype Identification: SNaP shot reaction
As described previously, the c.94G>A polymorphism was analyzed using the SNaPshot technique with the automatic genetic analyzer (Applied Biosystems, Foster City, CA, U. S. A.). This method relies on the extension of a primer that ends one base short of a polymorphic site, with fluorescent labeled dideoxy nucleotides, which are complementarily incorporated according to the sequence of the amplified target. The SNaPshot mixtures consisted of 5 uL of SNaPshot Multiplex Ready Reaction reagent (Applied Biosystems, Foster City, CA, U. S. A.), 5 pmol of SNaPshot primer (5'-CTAATCCCATGTACAATGCC-3'), and 3 uL of purified PCR product. The reaction was performed as follows: 25 cycles at 96℃ for 10 seconds, 50℃ for five seconds, and 60℃ for 30 seconds. After extension, the samples were treated with shrimp alkaline phosphatase. The samples were electrophoresed on an automated ABI PRISM 3100 genetic analyzer and analyzed with ABI GeneScan 3.1 analysis software (Applied Biosystems). Size determinations were performed using the GeneScan-120 LIZ size calibrator with Genotyper Version 2 data collection software.
Statistical Analysis
The frequencies of the genotypes and alleles of the polymorphisms were compared between NTG patients and the controls. The results were taken to be statistically significant when the p value was <0.05. For the Fisher's exact test, double-sided p-values were calculated using the sum of small p-values.14 The statistical analyses were performed using SPSS for Windows version 10.0 (SPSS Inc., Chicago, IL, U. S. A.). Conformance with the Hardy-Weinberg equilibrium for the genotype distributions was determined using the chi-square test for the goodness of fit.
Results
The characteristics of the NTG patients and the controls are presented in Table 2. No significant differences were found between the two groups in terms of age, gender ratio, and IOP. The family history of glaucoma was found in 14 NTG patients (20.3%). The mean deviation scores from program 30-2 of the Humphrey visual field analyzer implied moderate visual field defects in patients with NTG.
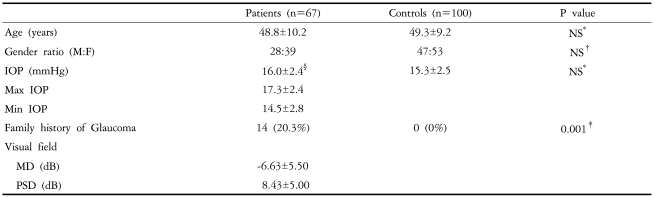
Characteristics of normal-tension glaucoma patients and controls
The genotype and allele frequencies of the polymorphisms in NTG patients (n=67) and controls (n=100) are shown in Table 3. In both groups, the genotype distributions were in accordance with the Hardy-Weinberg equilibrium. There was no significant difference in the frequency of the polymorphisms of Nppa and Npr1 gene alleles or genotypes between the NTG group and the control group. In the subgroup analysis of the age at diagnosis, there was no significant association between the Nppa and Npr1 genotype and NTG patients.
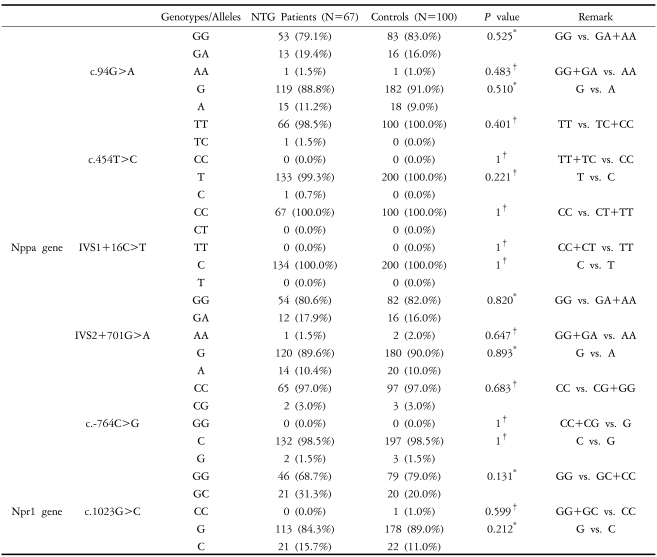
Genotype and allele frequencies
DISCUSSION
IOP is recognized as the only factor among multiple others responsible for optic nerve damage in glaucoma. But considerable evidence has been collected implicating vascular insufficiency as the cause of glaucomatous nerve fiber damage.15-18 The expression of NPs in the neural bundles of the anterior portion of optic nerves12 and their functions in regulating vessel tone and blood flow9 may suggest a possible role in the pathogenesis of glaucoma. This study investigated the association between NTG and the genetic variations of the Nppa and Npr1 gene.
NPs are potent vasodilators that may play a role in the pathogenesis of various vascular diseases such as hypertension. It has been suggested that NPs and their receptors in the human retina have a paracrine or autocrine function.12 NPs could also act as neurotransmitters or neuromodulators in the retina, as do other peptides such as vasoactive intestinal peptide or neuropeptide Y, which have effects similar to those of ANP.19,20 Interestingly, it has been suggested that ANP may contribute to cortical spreading depression-induced neuroprotection in the rat cerebral cortex, via effects on c-GMP production and other signal-transduction pathways.21
The c.454T>C polymorphism in exon 3 of the Nppa gene was previously known as the ScaI Nppa gene polymorphism because it can be detected by using ScaI restriction enzymes. It has been reported that this polymorphism has a significant association with nonfatal myocardial infarction, multiple-vessel coronary artery disease, hypertension, and microalbuminuria.22-29 Allele frequencies of the Nppa gene polymorphism have been reported to vary among ethnic groups. The frequency of the C allele is known to be 26.0% (n=50) in French Caucasians and 57.6% (n=48) in black Africans.30 In healthy subjects, the frequency of the C allele in Koreans is known to be 1.0% (n=180).31 In our study, its frequency was 1.5% (n=67) in NTG patients and 0.0% (n=100) in controls. The extremely low prevalence of Nppa polymorphism in our NTG and control subjects suggests this factor does not have a significant role in the pathogenesis of NTG.
IVS1+16C>T, IVS2+701G>A, c.-764C>G, and c.94G>A polymorphisms in the Nppa gene were reported to have significant associations with microalbuminuria, stroke, and hypertension.29,32,33 And the c.1023G>C mutation of the Npr1 gene-which is the missense mutation of methionine (ATG) to isoleucine (ATC) substitution at nucleotide 1023 in exon 3 of the Npr1 gene-may be associated with an increased risk for essential hypertension and myocardial infarction.34,35 In this study, the genotype distributions showed no significant differences between glaucoma patients and controls.
Tunny et al36 reported that no differences in the allelic frequencies of the c.454T>C and IVS2+701G>A polymorphisms in the Nppa gene were observed in primary open-angle glaucoma patients. But they also reported that PCR-SSCP analysis of the 5' proximal promoter region of this gene revealed mutations in 19% of the POAG patients in the -595 to -384 bp region. And he suggested that mutations in the 5' proximal promoter region of the Nppa gene might contribute to altered ANP transcription in at least a proportion of patients with familial glaucoma.
In cases of NTG, we could not find the association between the Nppa and Npr1 genotypes and NTG group. Because the genetic component is more important in the younger patients than in the older ones, our results in the relatively young NTG patients with mean age of 48.8 years indicate that other genetic factors might be involved in the development of this disease. However, the possibility of the association between NTG and other mutations or sequence changes in the Nppa and Npr1 gene cannot be excluded. The lack of an association between the common polymorphisms of the Nppa and Npr1 gene and NTG may suggest that this factor does not have a significant role in the pathogenesis of the optic neuropathy in NTG.
Notes
* This work was supported by Grant No. 04-2004-053-0 from the Seoul National University Hospital Research Fund.