

Macular coloboma are thought to result from incomplete differentiation of the arcuate bundles along the horizontal raphe during development; or they may result from intrauterine infection.1 Consideration of the differential diagnosis is essential because many diseases mimic a coloboma in the macula. Optical coherence tomography (OCT) may be a beneficial tool to make a diagnosis of macular coloboma, because it can show a subtle defect of the neurosensory retina and choroid at a higher resolution. However, due to the recent introduction of OCT, and the rare occurrence of macular coloboma, no data are currently available on its efficacy. We report on the OCT findings in a patient with unilateral macular coloboma. We are unaware of previous reports of these findings and could find no reference to it in a computerized search utilizing MEDLINE.
Case Report
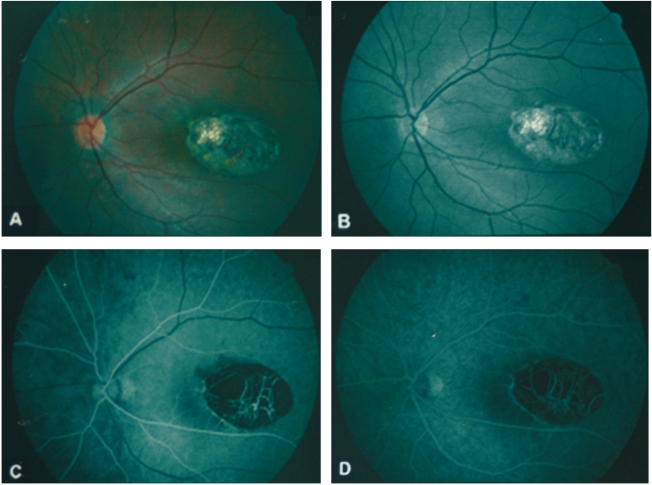
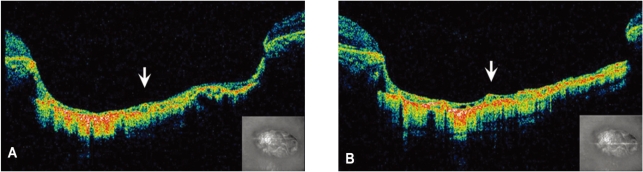
A 12-year-old boy was referred to our clinic for the evaluation of a macular lesion in the left eye. The past ocular and medical history was non-contributory. The best-corrected visual acuities were 20/20 in the right eye and 20/40 with -0.5 + 0.25 ├Ś 180 in the left eye. The anterior segment examination was unremarkable. The fundus examination of the left eye showed a sharply-demarcated, oval-shaped, excavated lesion involving the temporal half of the foveal center with large choroidal vessels and bared sclera at the base (Fig. 1A). The lesion was approximately four disc diameters (DD) in width and two DD in height, and the retinal vessels were undisturbed at the margin. On red-free retinal nerve fiber layer photography, papillomacular bundle were not interrupted surrounding the lesion (Fig. 1B). Fluorescein angiography (FA) showed hypofluorescence corresponding to the size of the lesion in both early and late frames without leakage of dye at any stage (Fig. 1C, 1D). The color vision test with the Titmus test and the visual evoked potentials were normal. The immunologic tests including toxoplasmosis, rubella, syphilis, cytomegalovirus, herpes virus and human immunodeficiency virus were all negative. The OCT (STRATUSOCT, Carl Zeiss Meditec, Inc., Dublin, CA) showed a crater-like depression accompanying atrophic neurosensory retina, and an absence of retinal pigment epithelium (RPE) and choroid in the lesion. Increased backscattering due to bare sclera and choroidal vessels were found (Fig. 2A, 2B).
Discussion
Ocular coloboma, defined as an absence of ocular tissue resulting from a failure of a part of the fetal fissure to close, is classified as atypical when it involves areas of the eye that do not originate from the embryonic cleft.1,2 Macular coloboma, classified as an atypical coloboma, can be present unilaterally or bilaterally. Although macular coloboma has a characteristic appearance and location, it must be differentiated from post-inflammatory scarring resulting from ocular toxoplasmosis or macular dystrophies.3,4 Sharma et al. evaluated a case of macular coloboma and provided histological evidence that these areas lacked choriocapillaries and RPE.5 The OCT performs cross-sectional imaging of biological tissue, similar to a histological section, at a resolution of 10 to 20 ┬Ąm, and thus can be beneficial for the diagnosis of macular coloboma without histologic section. In our study, we reported an OCT finding in a case of macular coloboma where we found an abnormal thinning of neurosensory retina, and an absence of RPE and choroidal tissue, leaving bared sclera in the lesion on the OCT.
Currently, a new generation of ultra-high resolution OCT technology has been introduced, using a femtosecond laser as the light source for imaging and achieving an axial image resolution of ~3 ┬Ąm. So, further study, using more advanced technology of OCT, would be helpful for definitely differentiating macular coloboma from other causes of macular pathology such as macular dystrophies and macular degeneration secondary to inflammation.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






