A Case of Scar Sarcoidosis of The Eyelid
Article information
Abstract
Purpose
We report the case of a patient with scar sarcoidosis that developed along a previous eyelid scar. There was no evidence of ocular or systemic sarcoidosis.
Methods
A 29-year-old man presented with a mass on his right eyelid that had been present for two month. On ocular examination an erythematous, firm, and non-tender mass was diffusely palpable along the upper and lower eyelid scar. We performed an incisional biopsy of the lower lid mass.
Results
Histopathologic examination of the mass revealed numerous, noncaseating granulomas with multi-nucleated giant cells. The giant cells contained asteroid bodies and calcium oxalate crystals characteristic of sarcoidosis, although the patient had no other evidence of systemic sarcoidosis. The mass in the upper lid disappeared after intralesional triamcinolone injections.
Conclusions
This case represents a rare occurrence of sarcoidosis that arose in an old eyelid scar. Scar sarcoidosis should be considered in the differential diagnosis of an unusual mass in a scar.
Sarcoidosis is a multisystem disorder, the cause of which is unknown, although it is characterized by a noncaseating, inflammatory granuloma.1,2 A scar sarcoidosis is a circumscribed form of cutaneous sarcoidosis localized in scars and is marked by inflammatory infiltrations and a livid discoloration. The occurrence of scar sarcoidosis has been described after conditions, such as herpes zoster infections,3 and masses have been reported to arise at previous scars caused by venepuncture,4 operations, trauma, cosmetic tattoos, traumatic tattoos,5 as well as at sites of previous laser surgery.6 Here we report an unusual case of scar sarcoidosis of the eyelid.
Case Report
A previously healthy 29-year-old man presented with a 2-month history of a mass that had arose in an old scar on his right eyelid. The scar dated back to a traffic accident that happened more than eight years prior.
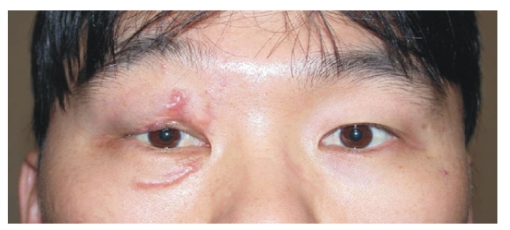
An ocular examination was performed, and an erythematous, firm, and non-tender mass was diffusely palpable along the upper and lower eyelid scar (Fig. 1).

An erythematous firm mass is visible along the upper and lower eyelid scar.
We performed an incisional biopsy of the mass on the patient's lower eyelid. Histopathologic examination revealed numerous, noncaseating granulomas with multi-nucleated giant cells, surrounded by relatively few lymphocytes (Fig. 2). The giant cells contained asteroid bodies and calcium oxalate crystals, characteristic of sarcoidosis (Fig. 3, 4). Ziehl-Neelsen staining failed to locate any acid-fast bacilli, and GMS (Gomori methenamine acid) staining ruled out the presence of fungal organisms. In addition, polarizing light microscopy did not reveal any foreign material. Laboratory studies were performed, but failed to demonstrate any evidence of systemic sarcoidosis.

A photomicrograph of the biopsy showing the numerous, noncaseating granulomas with multi-nucleated giant cells, surrounded by lymphocytes. (hematoxylin and eosin stain, ×200)
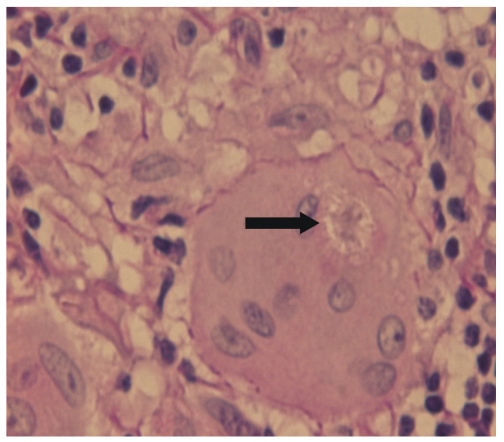
A photomicrograph of the biopsy showing the giant cells containing asteroid bodies (arrow). (hematoxylin and eosin stain, ×400)

A photomicrograph of the biopsy showing the calcium oxalate crystals (arrow). (hematoxylin and eosin stain, ×200)
Intralesional triamcinolone (4 mg/0.1 cc) 0.6 cc was injected in several fractions at 1-cm intervals along the upper lid mass. After one month, there was dramatic resolution of the lesions in the area that received treatment (Fig. 5). An additional dose of 1cc triamcinolone was injected in the masses of the upper and lower lids two months after the first injection. No palpable mass was present one year after the treatment.
One month after triamcinolone injection, there was a dramatic resolution of the lesions of the upper lid mass.
Discussion
A diagnosis of sarcoidosis is made by exclusion, whereby any infectious etiologies, including fungi, mycobacteria, and spirochetes, have been ruled-out. In addition, the differential diagnosis for sarcoidosis includes tuberculoid leprosy, Crohn's disease, and rosacea, as well as foreign body granulomatous diseases, such as silicosis. Although there is cutaneous involvement in approximately 25% of patients with sarcoid osis, few reports in the ophthalmic literature describe sarcoidosis of the eyelid skin.7,8 Most patients who present with scar sarcoidosis also have systemic sarcoidosis, and most patients also have pulmonary involvement, including bilateral hilar lymphadenopathy and restrictive pulmonary disease.
To the best of our knowledge, this is the first reported case of scar sarcoidosis of the eyelid in the ophthalmic literature. Although several cases of isolated cutaneous involvement of sarcoidosis have been documented,6,9 this case is unique and certainly unusual, in that no evidence of any systemic involvement was identified.
It is not clear whether previously inactive scars can develop the features of sarcoidosis as a result of primary systemic sarcoidosis. Nor it is clear, whether isolated cases of cutaneous sarcoidosis without systemic involvement are a separate disease entity. However, Ingber & Klinken demonstrated that scar sarcoidosis can be an early sign of systemic sarcoidosis.10 In order to better understand the pathophysiology and progression of cutaneous sarcoidosis, further studies are needed.
Sarcoidosis of the eyelid should be treated if the lesions are cosmetically disfiguring or if they interfere with eyelid function. The therapeutic approaches range from application of topical, intralesional, and/or systemic corticosteroids to the systemic administration of cytostatic drugs, chloroquine, vitamin D, allopurinol, and thalidomide. In addition, intralesional corticosteroid injections have been used for many years for a variety of inflammatory skin diseases, including sarcoidosis. In the case presented here, we found that the scar sarcoidosis responded dramatically to intralesional triamcinolone injection.
This case represents a rare occurrence of sarcoidosis that arose in an old eyelid scar. We conclude that scar sarcoidosis should be considered in the differential diagnosis of an unusual mass present in a scar.