Different Number of Sessions of Intense Pulsed Light and Meibomian Gland Expression Combination Therapy for Meibomian Gland Dysfunction
Article information
Abstract
Purpose
To evaluate the effect of the intense pulsed light (IPL) and meibomian gland (MG) expression (MGX) combination therapy according to the total numbers of sessions in the meibomian gland dysfunction (MGD).
Methods
Ninety patients with MGD were included. Patients had maximal five sessions of IPL (Aqua Cel, Jeisys Medical) and MGX combination therapy at 2-week intervals. The ocular surface disease index (OSDI) questionnaire score, MG profile grades, tear matrix metalloproteinase-9 (MMP-9), tear break-up time (BUT), tear osmolarity, tear secretion, and corneal erosions were evaluated.
Results
The number of patients who had a total of one to five sessions (1S to 5S) was 10, 25, 17, 20, and 18, respectively. The time-serial decrease of OSDI scores was significant in patients who had three or more sessions (3S, p = 0.002; 4S, p < 0.001; 5S, p < 0.001). The MG expressibility grade decreased with two or more sessions (2S–5S, p < 0.001), but the meibum quality significantly improved with all sessions (1S, p = 0.012; 2S, p = 0.024; 3S, p = 0.015; 4S, p < 0.001; 5S, p < 0.001). Although tear BUT increased even in patients with one session (1S, p = 0.040; 3S, p = 0.005; 4S, p = 0.006; 5S, p = 0.021), tear MMP-9, osmolarity, Schirmer I, and corneal erosions were not improved in every number of sessions. The female sex was the sole contributor to the final symptomatic improvement (p = 0.042), and the MGD stages were not related to the final OSDI decrease.
Conclusions
The OSDI score, MGD grades, and BUT were improved after the IPL and MGX combination therapy in MGD patients. Unlike MGD grades and tear film instability might be improved just after a few sessions, the overall subjective relief was accomplished in three or more sessions.
Dry eye disease (DED) is commonly seen in ophthalmic outpatient clinics and its prevalence ranges from approximately 5% to 50% worldwide [1]. It is known that a substantial proportion of DED patients accompany meibomian gland (MG) dysfunction (MGD), which is a leading cause of evaporative type DED [2]. The treatment of MGD is often challenging since the pathogenesis is multifactorial and MGD leads to variable symptoms of pain, irritation, and visual discomfort [2,3]. As it was well described that symptoms in DED were poorly correlated [4,5], the discordance between symptoms and signs of MGD makes doctors confused and intimidated to make therapeutic strategies [6].
Conventional treatments for MGD start from warm compression of the lid in conjunction with lid hygiene improvement most importantly and also include the use of artificial tears, anti-inflammatory eye drops, or oral medication [2]. However, there are limitations of these daily treatments because all of them rely hard on the patients’ efforts, requiring continuous participation from them. Unfortunately, compliance with basic eyelid hygiene therapy was once reported to be 55% [7], and some anti-inflammatory eye drops can be easily quitted because of discomfort in the eyes with the estimated prevalence of 2.5% to 60.0% [8–10]. In addition, oral medicines like omega-3 or tetracycline antibiotics pose more problems since they can cause gastrointestinal problems. Given that self-treatment may detract from long-term compliance, a real-world interventional treatment of MGD that lessens the time and mental burden of self-treatments will be beneficial.
Intense pulsed light (IPL) therapy came up to be used in treating MGD recently [11,12]. IPL therapy applies arrays of wavelengths of light on the eyelids to exert heating in the obstructed meibomian glands and to lead to anti-inflammatory effects by damaging the inflamed subcutaneous vessels in MGD [11]. Moreover, recent several clinical trials revealed the therapeutic efficacy of the protocolized IPL therapy combined with the meibomian gland expression (MGX) for the treatment of MGD [13–16]. Although those studies set up the fixed regular, steady, and continuous IPL treatment protocol to evaluate its therapeutic efficacy, in real-world situations, the rapid symptomatic improvement or the patient’s dissatisfaction with the treatment might terminate the protocol early unexpectedly. Furthermore, there is not an established optimal number of IPL treatments in MGD yet and numerous trials suggest their protocols instead which are quite different from each other [11].
In this regard, we included a real-world retrospective cohort who had different total numbers of sessions of IPL therapy combined with MGX for the management of MGD. In the cohort, we evaluated the time-serial effect of the combination therapy. Then, the subjective and objective parameter improvement was analyzed according to the total number of sessions.
Materials and Methods
Ethics statement
This study was approved by the Institutional Review Board of Chung-Ang University Hospital (No. 2107-024-19375) and adhered to the tenets of the Declaration of Helsinki. The Institutional Review Board waived the need for informed consent due to the retrospective nature of the study.
Study design
Patients who presented MGD in Chung-Ang University Hospital between November 2020 and March 2021 and who were treated according to our management method for MGD treatment were included in this study. This was a single-arm study based on the retrospective medical chart review.
MGD evaluation
Evaluation for MGD was done through dynamic and static observation of meibomian glands at the upper lids: (1) dynamic observation of meibum expressibility throughout MG orifices (i.e., MG expressibility grade), (2) dynamic observation of meibum quality (i.e., meibum quality grade), and (3) static observation of lid margin vascularity (i.e., lid margin vascularity grade). MG expressibility grade was evaluated with firm digital pressure at upper central lid margin and was graded from 0 to 3: 0, all glands expressible; 1, three to four glands expressible; 2, one to two glands expressible; 3, no glands expressible [17,18]. Meibum quality was graded from 0 to 3 after squeezing upper central meibomian glands: 0, clear secretion; 1, cloudy fluid; 2, cloudy particulate fluid; 3, toothpaste-like expression [18]. Lid margin vascularity was graded from 0 to 3 based on the degree of redness in the lid margin and the distribution of telangiectasia crossing meibomian gland orifices using standard photographs as provided in a previous report [19]. The severity of MGD was subdivided into stages 1 to 4 based on the clinical signs as previously established [20]. The more severe eye was selected to decide the MGD stage in the patient.
IPL and MGX combination therapy with concurrent medication
The method for the IPL and MGX combination therapy-based MGD treatment is summarized in Fig. 1. Our method is mainly based on the repetitive IPL and MGX combination therapy combined with a flexible regimen of concurrent medication of minocycline and/or diquafosol sodium and steroid eye drops. We performed IPL and MGX therapy in patients who revealed MGD in both eyes according to the dynamic grading (MG expressibility grade ≥1 and/or meibum quality grade ≥1) and who has at least one of the following four types of occasional ocular discomfort: foreign body sensation, ocular pain, visual discomfort, and ocular surface irritation. Patients with a systemic immunologic disease, the use of antiglaucomatous eye drops, and a history of contact lens wear within the previous 3 months were excluded from this retrospective study.
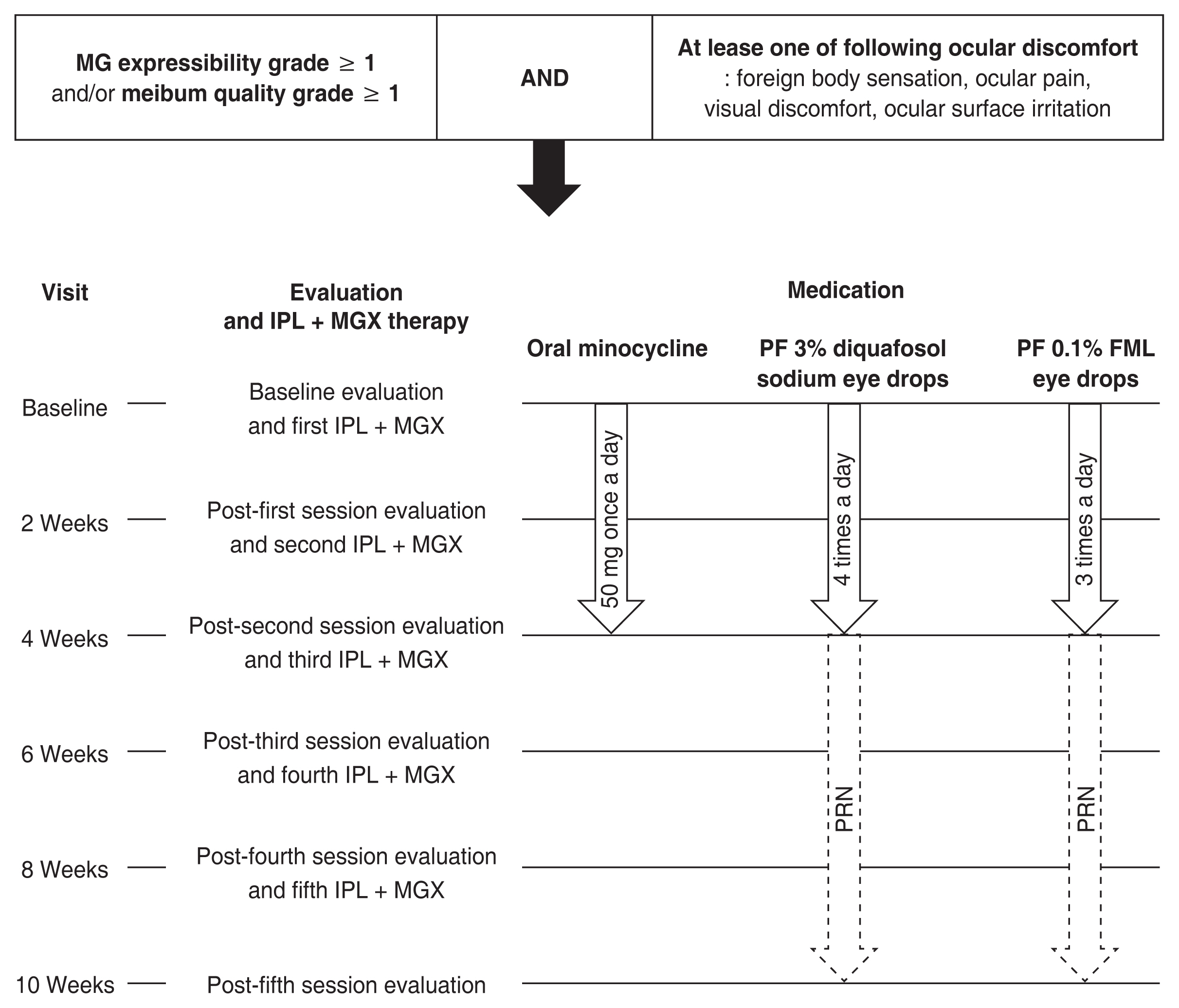
The serial intense pulsed light (IPL) and meibomian gland (MG) expression (MGX) combination therapy-based management method of MG dysfunction (MGD). The MGD treatment in this study is composed of a maximum of five sessions of IPL and MGX combination therapy at 2-week intervals with concurrent medications including oral intake of minocycline and preservative-free (PF) 3% diquafosol sodium eye drops and PF 0.1% fluorometholone (FML) eye drops. Clinical evaluation of ocular parameters for MGD was performed at 2-week intervals. PRN = pro re nata.
At the time of starting the treatment, we evaluated baseline conditions of subjective and objective ocular parameters for MGD, then we proposed patients undergo a maximum of five sessions of IPL and MGX combination therapy every 2 weeks starting the first treatment on the first visit. The total number of treatment sessions was flexible depending on the patients’ intention according to their postsession satisfaction after the IPL and MGX combination therapy. At each visit, patients could decide whether to continue the session according to the symptomatic improvement. As for eye drops, patients were educated to drop 3 % preservative-free diquafosol sodium eye drop (Diquas-S; Santen, Osaka, Japan) four times a day and preservative-free 0.1 % fluorometholone eye drop (Fumelon; Hanlim, Yongin, Korea) three times a day in both eyes for 1 month. Also, oral minocycline 50 mg was prescribed once a day only for 1 month which was a dose-attenuated regimen unlike the preestablished regimen of 50 mg twice a day in MGD [21]. If patients had a gastrointestinal problem and did not want to take pills, they were allowed not to take minocycline. After 1 month, patients were recommended to drop both eye drops only pro re nata (PRN) when they have dryness or ocular discomfort. Patients were asked to revisit 2 weeks after the last treatment session of IPL and MGX regardless of the total number of treatment sessions to evaluate the final check-up for MGD conditions after the treatment.
Evaluation of subjective and objective ocular parameters for MGD
Both subjective and objective conditions in enrollees were evaluated at each visit. At every visit, the enrollees were asked to fill out an ocular surface disease index (OSDI) questionnaire [22] to assess their subjective ocular symptoms. Various objective ocular parameters were evaluated. MGD severity grades, the tear break-up time (BUT), tear secretion by Schirmer I test without anesthesia, and corneal erosions were evaluated at every visit. The tear matrix metalloproteinase-9 (MMP-9) expression in tear and tear osmolarity was evaluated at baseline, post-second, and post-fourth treatment sessions. Tear BUT was measured after a drop of normal saline which was put on strip paper coated with fluorescein dye (Haag-Streit, Koniz, Switzerland) applied to the inferior fornix, and stained tear film. The time when the first break of tear film was observed under cobalt blue filter after the last blinking was considered as tear BUT. Schirmer I test was used for the evaluation of tear secretion. Schirmer standard strip (Eagle Vision, Memphis, TN, USA) was applied on the outer one-third point of lower conjunctival fornix and absorbed tear fluid for 5 minutes without analgesia. For ocular staining score, each eye went through slit-lamp examination under a yellow filter after fluorescein instillation. Corneal erosions were evaluated according to the National Eye Institute (NEI) scoring system [23]. The test for tear MMP-9 was done with a point-of-care immunoassay kit (InflammaDry; Quidel, San Diego, CA, USA) which was previously demonstrated to properly diagnose inflammation related to dry eye, following instructions from product documentation. Tear MMP-9 expression was graded from 0 to 4 based on a five-stage grading system [24]. To measure tear osmolarity, the test strip of I-PEN (I-MED Pharma Inc., Montreal, Canada) was soaked with tear at the lower conjunctival fornix and assembled into an analyzer that shows a test result in digits.
The examination for objective assessments of clinical parameters was performed in order listed as previously reported [25]: tear osmolarity, tear MMP-9, tear secretion with Schirmer I without anesthesia, tear BUT, corneal erosion score using fluorescein dye, MG expressibility, lid margin vascularity, and meibum quality of the secreted meibum.
Method of the performance of IPL therapy
IPL therapy was performed with a newly launched machine in Korea (Aqua Cel; Jeisys Medical, Seoul, Korea) which has a 590 nm cutoff filter only for MGD treatment and emits three-pulsed light per shot. Aqua Cel features an automatic temperature control device inside a handpiece which enables setting a wanted temperature at the surface of IPL crystal. Our institutional IPL manual is described in Fig. 2. At each treatment session, a cornea-protective silicone shield was inserted after topical anesthesia and the ultrasonic gel was applied to the treatment area at the upper and lower eyelids. The intensity of IPL was first determined as 16 J/cm2 and 15 J/cm2 in Fitzpatrick skin type III and IV, respectively. If a patient had pain at the first shot within a treatment session, the intensity was then lower to a range of 13 to 15 J/cm2 and 12 to 14 J/cm2 in Fitzpatrick skin type III and IV, respectively. Once an intensity was determined, it was fixed over entire steps in the patient within a session. The IPL manual is composed of four steps of IPL treatment followed by MGX (Fig. 2). In step 1, the five vertically oriented shots were applied from the main IPL crystal (44 mm [length] × 11 mm [width] × 11 mm [height]) at the lower eyelid area from nasal to temporal area two times. In step 2, the two horizontally oriented and overlapped shots were applied from the main IPL crystal at the area over a lower tarsus one time. In step 3, the small-sized but tall-tip cover (15 mm [length] × 9 mm [width] × 11 mm [height]) was put on the main IPL crystal and three shots were applied over an upper tarsus two times. In step 4, the same three shots within step 3 were applied over a lower tarsus one time. Every shot was applied very near the lid margin in all steps. The IPL therapy was performed bilaterally in all patients. Then, MGX was performed on both the upper and lower eyelids of each eye with compressor forceps.
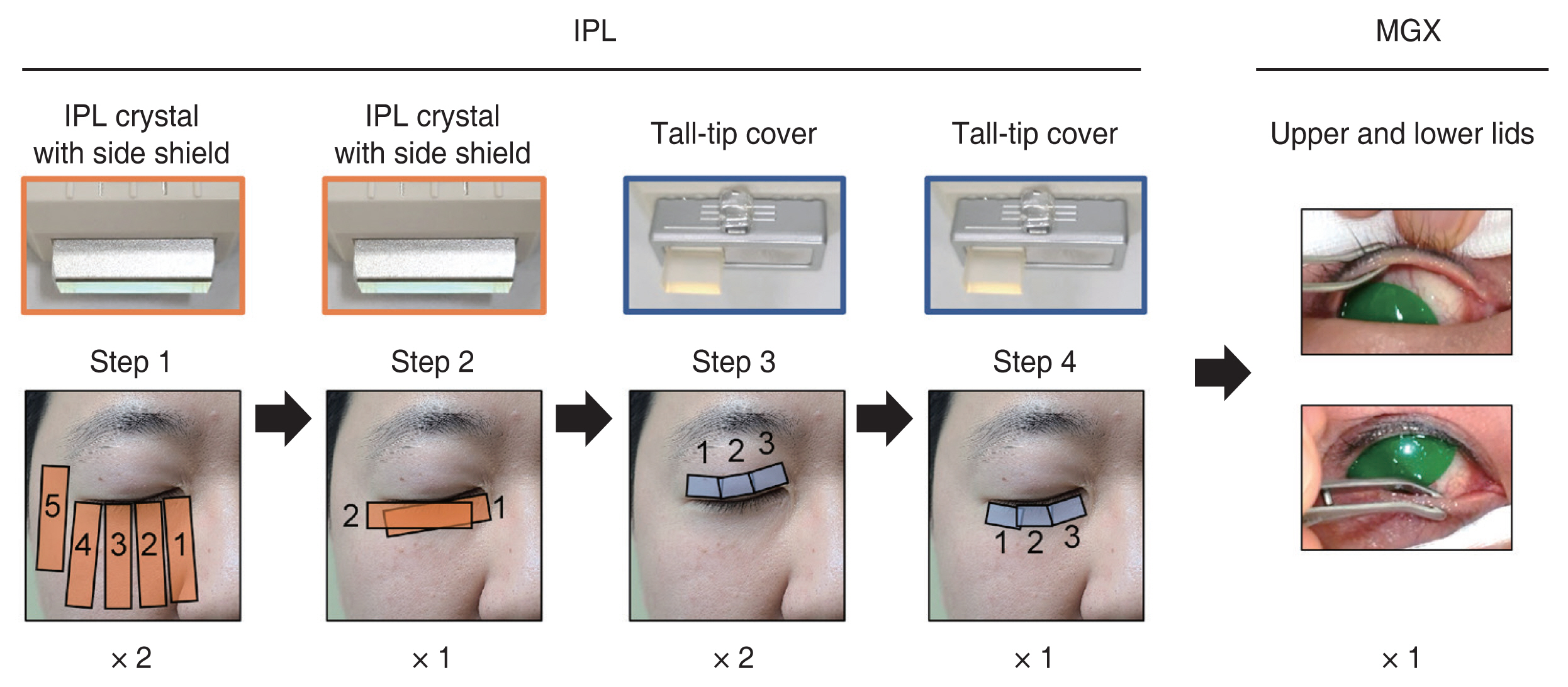
Manual for the performance of intense pulsed light (IPL) therapy for patients with meibomian gland dysfunction. The IPL machine is composed of four steps of IPL treatment followed by meibomian gland expression (MGX). In the first two steps, the main IPL crystal in the handpiece was used for shots, then a tall-tip cover was covered over the IPL crystal in steps 3 and 4. In step 1, the five vertically oriented shots were applied from IPL crystal at the lower eyelid area from nasal to temporal area two times. In step 2, the two horizontally oriented and overlapped shots were applied from IPL crystal at the area over a lower tarsus one time. Three shots were applied from a tall-tip over an upper tarsus two times in step 3 and over a lower tarsus one time in step 4. MGX was performed on both the upper and lower eyelids of each eye with compressor forceps. Informed consent for publication of the clinical images was obtained from the patient.
Design of outcome analyses
The main two axes of the outcome analysis were as follows: (1) consecutive changes of subjective and objective parameters according to the total number of sessions of IPL and MGX combination therapy; (2) identification of factors affecting the symptomatic improvement after IPL and MGX combination therapy.
It was defined that the subjective improvement was accomplished when the OSDI score after the final session of treatment decreased compared to the baseline score.
Statistical analyses
IBM SPSS ver. 26 (IBM Corp., Armonk, NY, USA) and Prism ver. 8.4.3 (GraphPad, La Jolla, CA, USA) were used for the statistical tests. The difference between the independent two groups was analyzed using the parametric Student t-test or the nonparametric Mann-Whitney U-test according to the normal distribution of the data. The intergroup difference among more than the two independent groups was analyzed using the Kruskal-Wallis test with Dunn’s post hoc. In patients who had a total of one session of treatment, the peritreatment change of parameters was analyzed using Wilcoxon signed-rank test. In patients who had a total of two or more sessions, the time-serial change of parameters was analyzed using one-way repeated measures analysis of variance, and the difference at each time point compared to the baseline was further evaluated by Bonferroni’s post hoc analysis. To compare continuous variables between two independent groups, a parametric two-tailed Student t-test or nonparametric Mann-Whitney U-test according to the normal distribution of the data. To compare categorical variables between groups, the chi-square test was used. A logistic regression analysis test was used to identify the contributing factors to the final improvement of OSDI scores after the final session. The data are expressed as mean ± standard deviation, and the differences were considered statistically significant at p < 0.05.
Results
Demographics and baseline evaluation
The demographic data are shown in Table 1. A total of 90 patients were included in this study. The 19 (21%), 20 (22%), 48 (53%), and three patients (3%) had MGD with severity stages 1 to 4, respectively. 80% were female and the mean age of total patients was 59.5 ± 11.6 years. At baseline state, the OSDI questionnaire score was 33 or higher in 58 patients (64.4%) of the total, which was classified as a severe subgroup based on a preestablished severity scale [26]. The mean OSDI score of total patients was 41.1 ± 24.4. MG profile grades revealed 1.5 ± 0.6, 1.6 ± 0.6, and 1.3 ± 0.8 according to the grading system of MG expressibility, meibum quality, and lid margin vascularity, respectively. Tear MMP-9 grade was averaged to 1.2 ± 1.0, tear BUT was 6.6 ± 2.3 seconds, and tear osmolarity was 312.4 ± 21.1 mOsm/L. Tear secretion by Schirmer I without anesthesia and corneal erosions were relatively normal.

Demographics and baseline clinical data of total patients
The number of patients who treated with a total one, two, three, four, five sessions of IPL and MGX combination therapy was 10 (11%), 25 (28%), 17 (19%), 20 (22%), and 18 (20%), respectively. The demographics and the baseline clinical data in patients according to the total number of treatments are shown in Table 2. The age, sex ratio, MGD severity stage, and clinical data except the tear MMP-9 grade were not different among the data from the five different sessions of treatment.

The difference in demographics and baseline clinical data of patients along with the total number of sessions of intense pulsed light and meibomian gland expression combination therapy
Changes in ocular parameters after treatment
First, to evaluate the change of values after each session of IPL and MGX combination therapy in the whole patient, we pooled the data from the whole patient with different numbers of treatment sessions. Then, the values after each session (baseline: 90 patients, 180 eyes; post-first session: 90 patients, 180 eyes; post-second session: 80 patients, 160 eyes; post-third session: 55 patients, 110 eyes; post-fourth session: 38 patients, 76 eyes; post-fifth session: 18 patients, 36 eyes) were compared to values at the baseline. Such pooling data revealed that the OSDI score, MG profile grades, tear MMP-9 grades, and tear BUT were improved during the treatment session compared to the baseline. The mean OSDI scores decreased after the third session (p < 0.05) (Fig. 3A). The dynamic MG profile grades continued to decrease compared to baseline significantly after every treatment session (all p < 0.001) (Fig. 3B, 3C). The lid margin vascularity grades improved after the second and third sessions (each p < 0.01) (Fig. 3D), and tear MMP-9 grades decreased after the fourth session ( p < 0.001) (Fig. 3E). Tear BUT continued to increase until after the fourth session compared to the baseline (post-first session, p < 0.05; post-fourth session, p < 0.05; post-second session, p < 0.01; post-third session, p < 0.001) (Fig. 3F). Tear osmolarity, tear secretion by Schirmer I test, and corneal erosion scores did not show significant change at each session (Fig. 3G–3I).

Change of the symptomatic and objective parameters pooled from the whole 90 patients before and after the intense pulsed light and meibomian gland (MG) expression combination therapy. Serial results of (A) subjective discomfort in ocular surface disease index (OSDI) scores, MG profiles including (B) MG expressibility, (C) meibum quality, and (D) lid margin vascularity, (E) matrix metalloproteinase-9 (MMP-9) expression in tear, (F) tear break-up time (BUT), (G) tear osmolarity, (H) tear secretion by Schirmer I test without anesthesia, and (I) corneal staining scores before and after the serial treatment sessions. (A) Baseline (0 weeks), 90 patients; post-first session (2 weeks), 90 patients; post-second session (4 weeks), 80 patients; post-third session (6 weeks), 55 patients; post-fourth session (8 weeks), 38 patients; post-fifth session (10 weeks), 18 patients. (B–I) Baseline, 180 eyes; post-first session, 180 eyes; post-second session, 160 eyes; post-third session, 110 eyes; post-fourth session, 76 eyes; post-fifth session 36 eyes. Values represent the mean ± standard error of the mean. NEI = National Eye Institute. *p < 0.05; †p < 0.01; ‡p < 0.001 versus baseline (Kruskal-Wallis test and Dunn’s post hoc).
Then, we stratified the time-serial changes of parameters according to the total number of sessions of IPL and MGX combination therapies (i.e., one session [1S] to a maximum of five sessions [5S]). While OSDI score did not change serially in patients who had a total of one and two sessions of IPL and MGX combination therapies, patients who had a total of three or more sessions revealed time-serial symptomatic relief (3S, p = 0.002; 4S, p < 0.001; 5S, p < 0.001) (Table 3). The MG expressibility was improved in patients who were treated with two or more sessions (2S–5S, p < 0.001), and the meibum quality grade improved in any number of treatment sessions (1S, p = 0.012; 2S, p = 0.024; 3S, p = 0.015; 4S, p < 0.001; 5S, p < 0.001) (Table 4). Lid margin vascularity grade was improved only in patients with a total of one and two sessions (1S, p = 0.002; 2S, p = 0.021) (Table 4). While the time-serial improvement of tear BUT showed statistical significance in patients with the total of one, three, four, and five sessions (1S, p = 0.040; 3S, p = 0.005; 4S, p = 0.006; 5S, p = 0.021), other objective parameters did not show the consecutive improvement in all numbers of treatment sessions (Table 5).

The time-serial change of OSDI scores after the intense pulsed light and meibomian gland expression combination therapy according to the total number of sessions
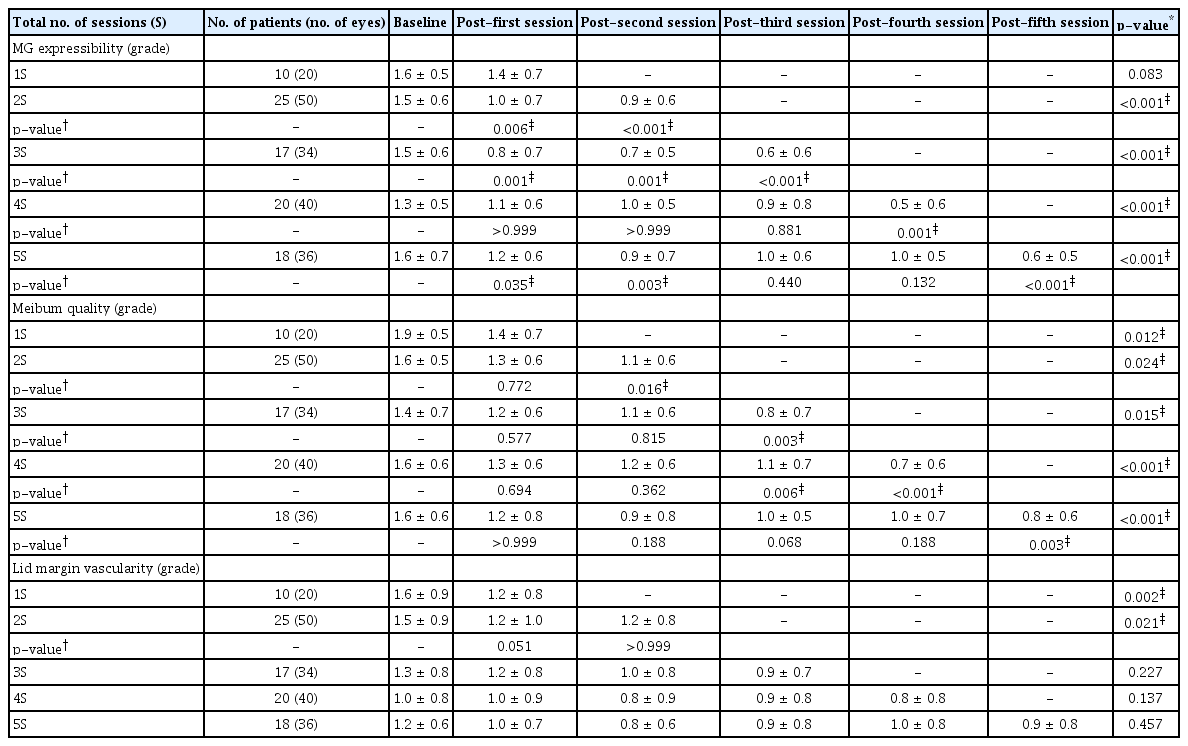
The time-serial change of MG profile grades after the intense pulsed light and MG expression combination therapy according to the total number of sessions of therapy.

The time-serial change of tear MMP-9 grades, tear BUT, tear osmolarity, tear secretion, and corneal erosion score after the intense pulsed light and meibomian gland expression combination therapy according to the total number of sessions
In our cohort, there was no skin burn or blister formation in the face except temporary erythema that was improved within a few hours. Hyperpigmentation occurred in three patients in the lower lid area after two to three treatment sessions but subsided over about 2 months spontaneously.
The difference in the baseline parameters according to the final symptomatic improvement
Next, we compared the difference in the demographics, the total number of sessions of treatment, the minocycline intake, and the baseline ocular parameters between patients with and without final symptomatic improvement represented by the decrease of OSDI scores after the consecutive IPL and MGX combination therapies. Thus, we further divided the patients into two subgroups; patients with improved OSDI scores (i.e., subgroup 1, n = 65) and patients with no improvement OSDI score after the last treatment session compared to baseline (i.e., subgroup 2, n = 35). The results are shown in Table 6. There was no significant difference in the total treatment sessions between subgroups. The mean age of patients was younger in subgroup 1 (subgroup 1, 58.0 ± 12.5 years; subgroup 2, 63.4 ± 7.7 years; p = 0.046). The initial intake of minocycline did not affect the symptomatic outcome after the protocol. The baseline OSDI score was higher in subgroup 1 (subgroup 1, 44.8 ± 23.5; subgroup 2, 31.7±24.6; p = 0.022) and the baseline tear MMP-9 grade was higher in subgroup 2 (subgroup 1, 1.1 ± 0.9; subgroup 2, 1.5 ± 1.2; p = 0.013). Other parameters at the baseline were not different between the subgroups.
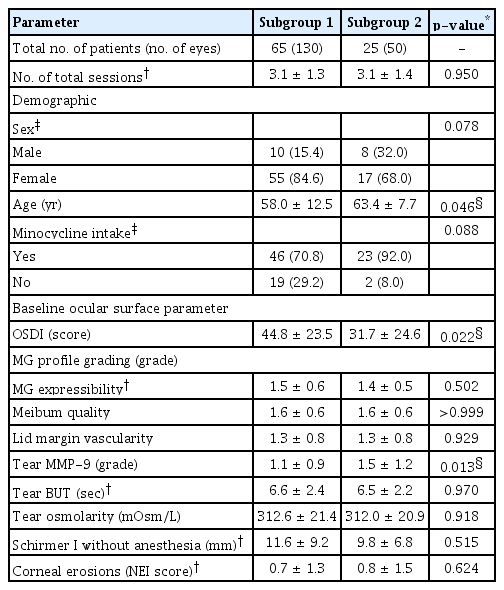
Difference of baseline clinical data according to the final improvement of subjective ocular discomfort
A logistic regression analysis, which was done to identify the contributing factors to the OSDI decrease after the final session of treatment, revealed that female sex was the sole factor in the final OSDI decrease after the IPL and MGX therapies (odds ratio, 80.786; p = 0.042). Age, the in-take of minocycline, baseline values of OSD score, MGD severity grades, tear MMP-9 grade, tear BUT, tear secretion, and corneal staining scores were not significant contributors.
The proportion of the patients with final subjective improvement was 79%, 60%, 73%, and 100% in MGD stages 1 to 4, respectively. There was no statistical difference in the ratio of patients with the final subjective relief among MGD severity stages (p = 0.379, chi-square test) (Table 7).

Difference in the proportion of the patient with the final subjective improvement after the consecutive intense pulsed light and meibomian gland expression combination therapy among the baseline severity of the MGD
Discussion
Numerous clinical trials recently reported the therapeutic effects of IPL with variable sessions in the treatment of MGD with concurrent additional treatments [11]. While the majority of studies performed three sessions [27–37] or four sessions [38–43] with 2-week or 4-week intervals, some reported that the efficacy of IPL therapies of even up to eight sessions [12,44] in MGD management. Despite that four sessions with a 3-week interval of IPL therapy are widely recognized now, we initially attempted a total of five sessions of treatment based on the variable sessions from the previous reports because the standard optimal session has not yet been established. We retrospectively included patients with MGD who had different numbers of IPL and MGX combination sessions up to five sessions with a 2-week interval. Then, we analyzed the time-serial improvement of both subjective and objective parameters in each total number of sessions. The OSDI score, dynamic MG profile grade, and tear BUT were improved in MGD after the consecutive sessions of IPL and MGX combination therapy. However, the overall subjective relief was accomplished in patients who had a total of three or more sessions unlike MG profiles, and tear film instability might be improved just after a few sessions.
Regarding IPL and MGX are intermittent treatments with a long interval and cannot be done at home as self-treatment, oral minocycline that was 50 mg once a day daily was prescribed for 1 month and patients were allowed to use diquafosol sodium and steroid eye drops to relieve the daily discomfort of MGD. Such use of concurrent medications may detract from the specific effect of IPL and MGX combination therapy which was usually seen through previous clinical trials [11]. However, it is hard to apply strict or fixed protocol over several months practically in clinics because patients usually want to stop or stop treatment by themselves after they became to feel better from their ocular discomfort. Furthermore, patients want to use simple eye drops preferentially or even already have used ophthalmic medication as needed (PRN). Patients either like or hate oral pills depending on their gastrointestinal conditions. Therefore, we wanted to reflect on the reality of situations for MGD treatments during the treatment in our cohort. In this regard, IPL and MGX combination therapy were stoppable before the completion of a maximum of five sessions when they felt subjective improvement and the usage of concurrent medication was flexible depending on their MGD-related symptoms.
At the baseline, there was no difference in demographics and values of parameters including dynamic and static MG profile grades, tear BUT, tear osmolarity, tear secretion, and corneal erosion score in all session number groups except tear MMP-9 (Table 2). Although the five-grading system from point-of-care MMP-9 immunoassay might reflect the gradual difference of concentration of MMP-9 in tear as previously investigated [24], the intergroup difference of tear MMP-9 might not always guarantee the real difference in MGD severity based on the essential semi-quantitative nature of the assay.
The time-serial subjective relief represented by the OSDI score decrease was seen in patients with a total of three or more sessions. However, we do not think that a minimum of three sessions of IPL and MGX therapies are essential to secure the symptomatic improvement in our treatment modality and method because patients with a total of three and four sessions of treatment already experienced symptom relief even after the first session (Table 3). In addition, there was no significant difference in the total number of sessions between subgroups with versus without the final OSDI improvement (Table 6). The drawback of the study design, which included a retrospective observational cohort in which patients are allowed to stop the consecutive sessions if they wanted to whether it was because of the rapid symptom improvement or the dissatisfactory response to the therapy, might have put in other factors beyond the treatment itself. Nevertheless, given that the OSDI scores continued to improve until the final in patients who had a total of three or more sessions and that the pooling data from the whole 90 patients revealed a significant decrease in OSDI scores especially after the third session compared to baseline, we think that the subjective improvement felt by the patient may not easily be achieved early during the consecutive treatment. Also, patients’ steady willingness to the consecutive therapies may contribute to the overall subjective improvement. But this issue must be verified in the prospective study with various groups randomly assigned to a different number of treatment sessions.
Intriguingly, MG profile grades and tear instability were improved even in patients with a total of one session of treatment (Tables 4, 5) unlike the OSDI results. This may be due to the multifactorial pathogenesis of MGD [3]. In addition, the different perception patterns of ocular surface-related discomfort verified by the OSDI questionnaire depending on the accompanying disease such as Sjögren’s syndrome [25] also suggest that the objective and subjective symptoms do not always go along with each other.
The tear BUT increased overall in the total of one, three, four, or five sessions groups, and the pooling data from tear MMP-9 grades from whole patients decreased after the fourth session in this study along with the subjective improvement. These results are concordant with previous studies which showed a decrease in tear levels of inflammatory cytokines, such as interleukin-6, interleukin-17, and tumor necrosis factor α, after IPL therapies and revealed the relation between these cytokines and MGD symptoms or MG profiles [28,35]. By contrast, at baseline, ocular surface erosions in the cornea were minimal and tear secretion was tolerable. Erosion scores and tear secretion did not change significantly after the completion of sessions compared to baseline. Such discordance suggests that the tear film instability or ocular surface inflammation might be major contributors to the ocular surface discomfort in our cohort of MGD patients. It is thought that the IPL therapy contributed to qualified lipid secretion from meibomian glands, and it resultantly helped in maintaining tear film by preventing tear evaporation.
We further tried to discover which factors were related to better symptomatic control after the IPL and MGX consecutive therapies and the female sex was the sole contributor to the positive response. Such a different subjective response to the IPL and MGX combination therapy may be hormonal and gender differences beyond the biological sex difference. Women’s healthcare-seeking behavior and health service utilization earlier as noted in DED [45,46] might have provided opportunities for early and active intervention to manage MGD. However, the statistical significance of sex as a contributor to the positive response was quite marginal (p = 0.042). The protocolized trial in subjects with the same MGD severity is needed to identify the definite demographics or the baseline ocular parameters to predict the favorable outcome after the IPL and MGX combination therapy.
The group with the final OSDI improvement showed patients with lower age, higher initial OSDI score, and lower baseline tear MMP-9 grade. The reasons for these factors are not fully understood. But we assume that since MGD is known to develop with the aging process [47], young patients’ MG would not be in fixed, structural deformities and remained capacity for improvement after treatment.
The intensity of IPL (Aqua Cel) was 15 to 16 J/cm2 in our cohort which was higher than a range of 11 to 14 J/cm2 from M22 IPL machine (Lumenis, Yokneam, Israel) in Asian patients [12], but nonetheless, there were no well-known adverse effects of IPL including skin burn, swelling, or blister formation [11] during the use of with Aqua Cel IPL. Aqua Cel allows higher energy intensity than other IPL machines with safety because its handpiece has a patented automatic temperature control device inside, which can keep cooling IPL crystal rapidly and efficiently. A recent retrospective study compared the effect between Aqua Cel and M22 devices in MGD patients and showed that both devices improved the Standard Patient Evaluation of Eye Dryness Questionnaire (SPEED) score, tear BUT, lid margin abnormalities, fluorescein staining, and meibum grade without significant differences [48]. Although the fluence and the total number of sessions were different and they did not accompany the MGX after the IPL treatment, our results of the subjective and objective improvement by AQUA CEL IPL therapy go along with the previous study [48].
It was recommended to evaluate the biochemical features of tears in DED from the more severe eye [49]. Also, the more severe eye may reflect the ocular discomfort better. However, given that IPL and MGX treatment was done independently in each eye and the objective parameters were evaluated separately, we included patients who had bilateral MGD, so who were performed with the IPL and MGX treatment in their both eyes. It is suggested that the random selection of one eye or the selection of more severe stage of eye may be preferred in a future study to correlate the subjective discomfort with ocular objective parameters after the IPL and MGX combination therapy.
This study has several limitations, which include: (1) a single-arm study based on retrospective data and (2) inhomogeneous treatment in the aspect of concurrent medications, severity stages of MGD, and the total number of IPL and MGX treatment sessions. Despite the limitation, this study merits in that we showed the therapeutic results in each total treatment session group and that we reported the different patterns of improvement between subjective and objective parameters within the same number of sessions. Moreover, we first report the therapeutic effect of Aqua Cel, a newly launched IPL machine for MGD treatment in Korea. A further prospective case-control study would give stronger evidence to the therapeutic results using the Aqua Cel IPL machine.
Although the overall subjective relief was accomplished in patients who had a total of three or more sessions in this study, our results do not show the optimal number of treatment sessions of IPL and MGX combination therapies. Recently, Toyos et al. [50] proposed four sessions of IPL and MGX combination therapy at 2-week interval in a randomized controlled study in MGD patients with moderate to severe symptoms. In this regard, the establishment of the optical protocol according to the IPL machine and to the severity of MGD will be one of the interesting candidate research topics.
In conclusion, we observed the time-serial therapeutic results of IPL and MGX combination therapy in MGD and compared the effect of symptomatic and objective parameter improvement according to the total number of sessions. Although the patients were not randomly assigned to the different total number of treatment sessions, the different patterns of change in OSDI scores according to the total number of sessions and the discrepancy of overall improvement between the objective and subjective parameters may guide clinicians to predict the short-term effect and to determine to continue the subsequent session during the MGD treatment.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: None.