


The human crystalline lens has a functional role in protecting the retina from ultraviolet (UV) phototoxicity apart from accommodation. UV light, which has a shorter wavelength than visible light, can be responsible for phototoxicity in retinal photoreceptors and pigment epithelial cells and can thus induce oxidative stress and damage [1,2]. UV light with wavelengths of shorter than 300 nm is mostly absorbed in the cornea [3], whereas UV light from 300 to 400 nm is usually absorbed in the crystalline lens depending on the degree of cataract. To prevent the retina from phototoxicity after cataract surgery, intraocular lenses (IOLs) with UV-light blocking properties are widely used in the clinic [4].
Blue light is a type of high-energy visible (HEV) light with wavelengths ranging from 400 to 500 nm. Under scotopic conditions, human eyes are known to see light with such wavelengths with the help of the rod cells’ sensitivity at this range of wavelengths [5]. In addition, the blue light also plays an important role in human circadian rhythm by affecting melatonin secretion of the pineal gland [6]. According to the latest research, blue light may, just as UV light, also cause phototoxicity in retinal photoreceptors and the pigment epithelium [2]. Various studies on the efficacy of blue light attenuation have been conducted, because light emitting diode light sources, which have been widely adopted in recent years, emit a lot of blue light [1,7-9]. In general, HEV light, often called “blue light,” is divided into the 400 to 440 nm violet spectrum and the 440 to 500 nm blue spectrum [9,10]. Of all blue light, the violet spectrum is known to cause more retinal phototoxicity while it has less effect on scotopic vision, contrast sensitivity, and circadian rhythm [4,7]. Therefore, there might be a need of IOLs that protect against the specific violet-light spectrum. In this study, several UV-filtering IOLs, UV- and blue-light filtering yellow-tinted IOLs, and the violet-light filtering IOL, which are widely used in clinical practice, are analyzed and compared in terms of light transmittance using a spectrophotometer.
Materials and Methods
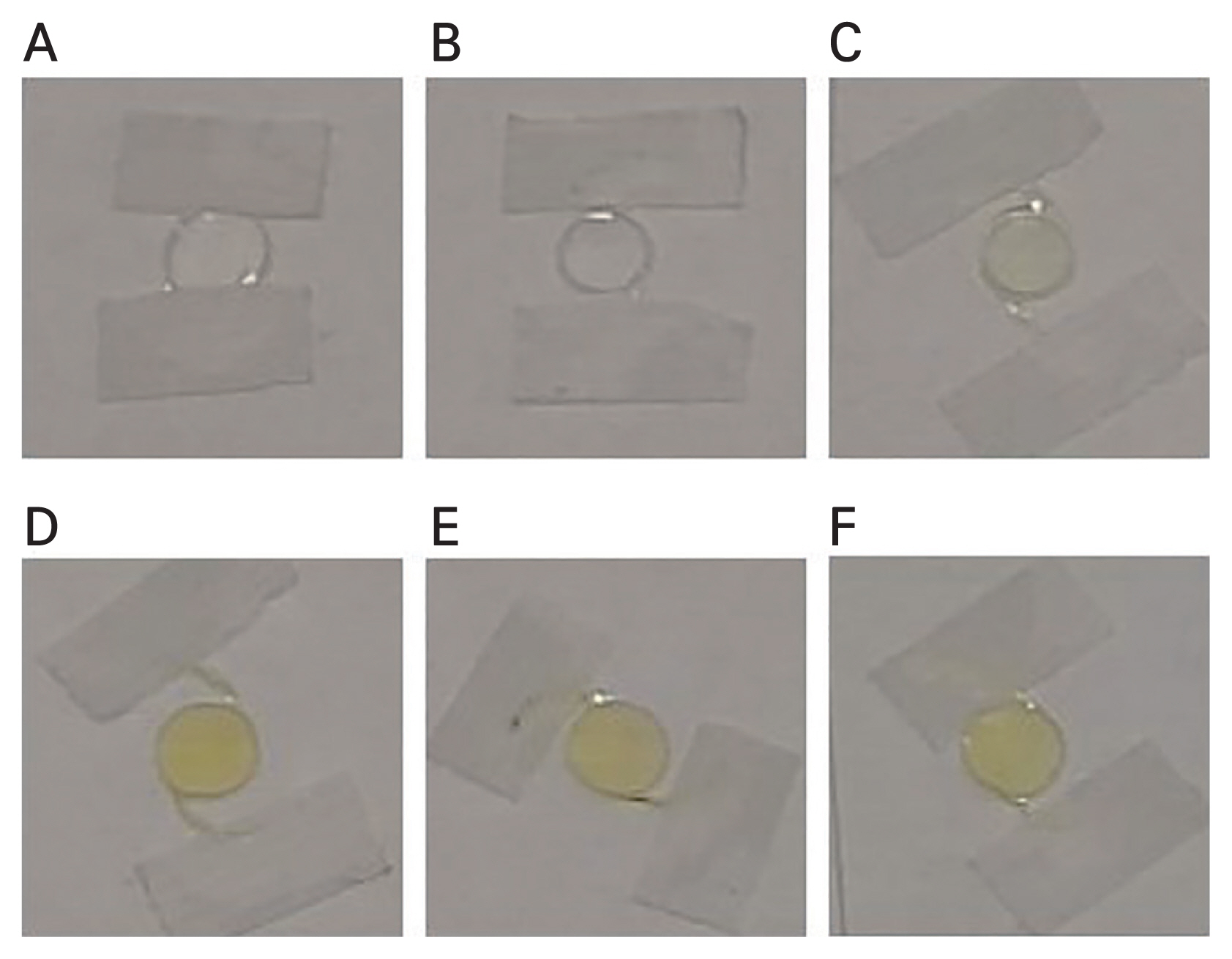
A total of seven IOL models were assessed with a spectrophotometer (Cary 5000 UV/VIS/NIR; Agilent technologies, Santa Clara, CA, USA), with high accuracy in wavelength analysis from UV wavelength (175 nm) to near-infrared (3,300 nm). The IOLs, a violet-light filter (Synergy ZFR00V; Johnson & Johnson, New Brunswick, NJ, USA), a UV-light filter (Tecnis ZCB00, Johnson & Johnson; XC1-SP, Hoya, Tokyo, Japan; and AT LISA 809M, Carl Zeiss, Jena, Germany), or a blue-light filter (yellow-tinted IOLs; Acrysof IQ SN60WF; PanOptix TNFT00; Alcon, Geneva, Switzerland; XY1, Hoya) were evaluated (Fig. 1). All the power of IOLs tested were 20.0 diopters to minimize experimental errors possibly due to a dioptric difference. Transparent glass panel was prepared for every IOL specimens. Each IOL’s haptics were fixed on transparent dry glass panel with optic position in parallel with the glass panel for spectrophotometry. The IOL specimens were then positioned under the spectrophotometer’s measuring beam with IOL’s optic center positioned to match the center of the reference beam. Each specimen was tested for its light transmission intensity (in %) and repeated five times. To eliminate confounding effect of panel glass, baseline transmission data with and without panel glass were measured and deducted from the specimens’ value. Then the mean values of all IOLs’ light transmission intensity were calculated for each wavelength in 1 nm units from 350 to 800 nm. The averaged values were displayed in a representative transmission curve.
Results
All UV-light filtering IOLs (ZCB00, XC1-SP, and AT LISA) showed an excellent absorption within the UV-light spectrum with wavelengths shorter than 400 mn. However, these IOLs showed no attenuation in the HEV light spectrum which is part of the visible light spectrum with wavelengths greater than 400 nm (Fig 2.).
Likewise, the yellow-tinted UV- and blue-light filtering IOLs (SN60WF, TNFT00, and XY1), showed a full protection from the UV-light (wavelengths shorter than 400nm). In the HEV light spectrum between 400 and 500 nm attenuations were achieved. In that range, the protection of the violet spectrum was higher than that of the blue spectrum.
The violet-light filter IOL (ZFR00V) steeply attenuated light with wavelengths under 430 nm compared to blue-light filtering IOLs and transmitted nearly all light with wavelengths of 440 nm or greater. The UV- and blue-light absorbing IOLs showed slow slope light-attenuating characteristics at wavelengths in the HEV light spectrum, whereas the violet-light filtering IOL and the UV-light filtering IOLs showed a tendency to rapidly increase the transmission at certain wavelengths (Table 1).
Discussion
In general, the wavelength of visible light is ranging from 400 to 700 nm and UV light is the range shorter than that. In recent studies, it has been discovered that HEV light with wavelengths ranging from 400 to 440 nm is potentially phototoxic to the retinal pigment epithelium of the retina, eventually which could lead to macular degeneration [2,8,10]. Due to the normal ageing process of the human crystalline lens, which gradually attenuates HEV light, the retina is protected from phototoxicity in mid-aged and older patients. In pseudophakic eyes, the macula can be exposed to retinal toxicity when all the wavelengths of the visible spectrum and ultraviolet light are transmitted [11].
A UV filtering function has been added to the majority of IOLs since 1980s. Later on, IOLs with a HEV light attenuation function have started to come out as many studies showed that HEV light may also have retinal toxicity. However, these yellow-tinted IOLs can have negative effects on patients’ contrast sensitivity, as they partially attenuate light within the visible spectrum. Especially the rod cell-mediated scotopic and mesopic vision relies also on the blue-light spectrum [7], Nakano et al. [4] compared surgery results with blue light-filtering IOLs and violet-light filtering IOLs. Patients who had received a violet-light filtering IOL achieved 3 months after surgery better results in terms of contrast sensitivity under photopic and mesopic conditions when compared with patients who had received blue light-filtering IOLs [4].
Furthermore, in natural environments, blue light has an inhibitory effect on melatonin secretion through a retinal melanopsin reaction by the pineal gland. Thus, during night-time with less blue light, melatonin secretion increases, which makes people sleepy. Therefore, blue light is involved in the human circadian rhythm. When such blue light is intentionally blocked, it can be expected to have a negative effect on the sleep cycle. However, in their study on a correlation between blue-light filtering IOLs and sleep quality, Feng et al. [6] discovered that there was no significant difference between patient groups who had received UV-light filtering IOLs or UV- and blue-light filtering IOLs. Both groups had better sleep quality after the surgery.
Violet-filtering IOLs specifically block HEV light with wavelengths shorter than 440 nm. This is different from the concept of blue-light filtering IOLs that broadly attenuate light with wavelengths between 400 and 500 nm. One of the main advantages of the violet-light filtering IOLs compared to blue-light filtering IOLs might be that they have less influence on light with wavelengths around 498 nm and improved scotopic vision can be expected because this could be the peak area of the rod cells’ activity [5,9]. However, this has not yet been demonstrated in an in vivo study.
In this study, we compared the three different blue-filtering IOLs. Two IOLs (SN60WF and TNFT00) were made of same material, having different optical properties, and XY1 was made of different material. Interestingly there was a difference in the characteristics of transmission of light with different materials. XY1 showed a much steeper curve in the 400 to 500 nm range, suggesting slightly better filtering profile in the range of 400 to 430 nm than SN60WF and TNFT00. Three blue-filtering IOLs did not show the complete filtering HEV light in the range of 400 to 430 nm and they did not allow full transmittance of blue and green light.
Violet-filtering IOL in this study showed much steeper curve than blue-filtering IOLs and it is quite similar degree of inclination to UV filtering IOLs. It was very effective in blocking the wavelength less than 430 nm and did not interfere with the transmission of light from 450 nm or more. So in real life situation after cataract surgery with this type of IOLs, we can expect more effective blocking of HEV light to retina and less interference of healthy blue and green light which is known to be necessary for physiologic condition and contrast sensitivity in scotopic vision.
The limitation of this study in terms of experiment settings were, we tested all the IOLs in dry condition and one of the tested IOLs showed the result of transmittance of UV light between 360 to 380 nm whereas all the others not. The only different characteristic of the IOL beside the color was hydrophilic nature, and tested that IOL in air-dried condition, so we need further testes of all models in same moisture chamber condition to compare each other.
In this study, violet-light filtering IOL showed a better transmittance characteristic, potential advantage to block high-energy wavelength which is known to have risk of reactive oxygen species damage to retinal pigment epithelium cells and allowing full transmission of healthy blue light compared to UV- and blue-light filtering IOLs. And we need further investigations in clinical aspect to confirm the violet-blocking IOLs can have such a superiority of contrast sensitivity in scotopic condition, circadian rhythms and sleep quality.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






