Recurrent Enterococcus faecalis Endophthalmitis Following Uneventful Cataract Surgery
Article information
Dear Editor,
We present a case of multiple recurrent Enterococus faecalis endophthalmitis after uneventful phacoemulsification and posterior chamber intraocular lens (IOL) implantation. This is an unusual condition, with only one previous published case [1].
A 77-year-old male with exfoliation syndrome and ocular hypertension had uneventful phacoemulsification at a primary eye care center in Sweden. Preoperatively, the periorbital skin and the eye were cleaned with chlorhexidine (5 and 0.5 mg/mL, respectively). A standard IOL (Tecnis One Piece PCB00; Abbott Medical Optics, Santa Ana, CA, USA) was implanted in the capsular bag. At the end of the procedure intracameral cefuroxime 1 mg (10 mg/mL) was given.
On postoperative day 2 the patient had a sudden onset of pain. Visual acuity was hand motions and the lamp examination showed an intense conjunctival injection, edematous cornea and anterior chamber reaction with hypopyon. The pupil did not react to light and the fundus was not possible to examine visually. B-scan ultrasound showed hyperreflective material in the vitreous chamber but no signs of retinal detachment. He received intravitreal vancomycin 1 mg (10 mg/mL). The following day a pars plana vitrectomy (PPV) was performed at a tertiary eye clinic 120 km away and 2 mg ceftadizim (20 mg/mL) was injected into the vitreous cavity. Inflammatory membranes were found adhesive to the retina. The patient received both topical (dexamethasone) and oral steroids (prednisolone). Three weeks after the PPV, the BCVA was Snellen 20 / 150. The intraocular pressure was around 30 mmHg, despite four different topical antiglaucoma medications (bimatoprost/timolol and brimonidin/brinzolamin).
On a scheduled control 5 weeks after the initial operation, the patient had hypopyon again and visual acuity had decreased to hand motions. He received intravitreal vancomycin 1 mg. The following day a second PPV was performed with intravitreal antibiotics: 1 mg vancomycin (2.3 mg ceftazidim (22.7 mg/mL) and 0.32 mg moxifloxacillin (1.6 mg/mL). At week ten, a YAG-laser iridotomy was performed due to iris bombé. The optic disc was pale and had a pronounced glaucomatous excavation. No inflammation was seen in fundus. As the pressure remained around 30 with five different topical antiglaucoma medications (apraklonidin added), a trabeculectomy with mitomycin-C was performed at week 20, which required needling with 5-flouracil at week 28.
Eight months after the initial surgery the patient had increased ocular pain, decreased vision to light perception and hypopyon. He received 1 mg intravitreal vancomycin and 2.3 mg ceftazidime (22.7 mg/mL) at the primary eye care center and the following day a third PPV was performed, and the eye was filled with silicone oil. The anterior chamber was injected with 1 mg cefuroxim (10 mg/mL) but no additional intravitreal antibiotics were given.
Eleven months after the initial surgery, the eye showed no signs of inflammation. The visual acuity was hand motion at 0.5 m.
E. faecalis was isolated in the vitreous specimen both from the initial incident and the two recurrences. Phenotypic antibiotic susceptibility testing demonstrated resistance to cefuroxime and ceftazidime but sensitivity to moxifloxacin and vancomycin. Whole genome sequencing was performed with isolates from all three incidents. Paired-end sequencing was made on the MiSeq (Illumina, San Diego, CA, USA), following library preparation using Nextera XT (Illumina). The SeqSphere software (Ridom, Münster, Germany) was used for de-novo assembly and core genome multi-locus sequence typing based on 1972 genes, resulting in one gene difference between isolate 2 and isolate 1+3. This indicates that the same strain caused all three infections.
Only six cases with recurrent Enterococcus endophthalmitis after phacoemulsification has been reported in the literature [2–5] and only one of them had two recurrences [1] (Table 1). In the present case the intravitreal injection of vancomycin was maybe washout by the following PPV. Still, the patient experienced a third episode of endophthalmitis despite intravitreal vancomycin followed by PPV with intravitreal vancomycin and moxifloxacin at the second activation. Formation of enterococcal biofilm on the IOL is one explanation [4]. Another is association with thin bleb wall after trabeculectomy or its needling. If patients with endophthalmitis are managed both at primary and tertiary eye clinics the full intravitreal regime of antibiotics should be repeated. In the case of recurrent endophthalmitis from E. faecalis, removal of the IOL or the use of silicon oil could be taken into consideration.
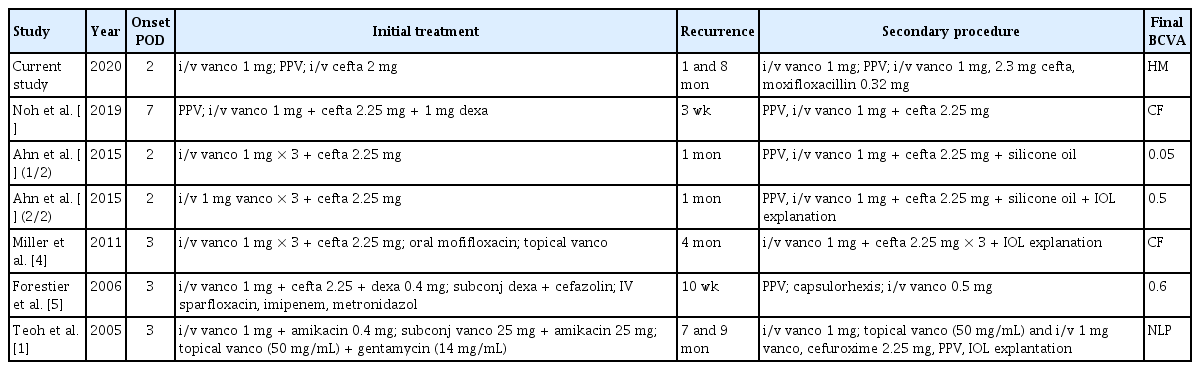
Cases of recurrent Enterococcus faecalis endophthalmitis after uneventful cataract surgery with phacoemulsification reported in the literature
Acknowledgements
This study was funded by Futurum Region Jönköpings län (FUTURUM-808791). We thank Sara Mernelius for laboratory analysis and Futurum Region Jönköpings län for valuable comments.
Notes
No potential conflict of interest relevant to this article was reported.