

Since McDonogh and Meiring [1] described the endoscopic transnasal dacryocystorhinostomy (DCR) procedure in 1989, various techniques and adjuncts have been used to enhance the success rate of the method [2,3,4]. Nevertheless, synechia formation between the lateral wall and the middle turbinate (or septum) is a common cause of endonasal DCR failure [5].
Various absorbable anti-adhesion agents have been used to prevent postoperative synechia formation after endonasal surgery [6,7,8]. Such agents prevent adhesion by forming a physical barrier to the surgical area and are then degraded and absorbed after the wound has healed. Hyaluronic acid (HA), a ubiquitous water-soluble polysaccharide component of extracellular matrix, is used as an anti-adhesion agent in a mixed form with less absorbable material like sodium carboxymethylcellulose [9]. A mixed solution of hyaluronate and sodium carboxymethylcellulose (Guardix-Sol) has been used intraoperatively as an anti-adhesion adjuvant after endoscopic sinus surgery [6] and endonasal DCR [10].
HyFence is a gel-type material that contains HA stabilized by 1, 4-butandiol diglycidyl ether, and Mediclore is a thermosensitive sol-gel anti-adhesion product composed of poloxamer, gelatin, and chitosan. Considering that the adhesion strength of anti-adhesion agents that can withstand gravity after injection into a surgical area is an important factor in endonasal surgery, both materials were expected to have advantages compared to Guardix-Sol.
However, no published reports have evaluated the anti-adhesion effect of HyFence or Mediclore after endonasal DCR; although Chang et al. [7] reported that HyFence had an equivalent anti-adhesion effect compared to Guardix-Sol in patients after endoscopic sinus surgery. To the best of our knowledge, this is the first reported attempt to evaluate the effects of HyFence and Mediclore after endonasal DCR compared to Guardix-Sol.
Materials and Methods
In this retrospective study, we performed a medical chart review of patients who underwent endonasal DCR using anti-adhesion adjuvant agents at the Seoul St. Mary's Hospital from March 2009 to February 2016. All patients signed an informed consent form for the surgical procedure. This study was approved by the institutional review board of the Catholic University of Korea (KC18RESI0585) and followed the Declaration of Helsinki.
All patients underwent complete ophthalmic examinations including eyelid evaluation, slit lamp examination, lacrimal irrigation, and nasal endoscopic evaluation. Patients were excluded if epiphora was caused by facial palsy or severe eyelid laxity. We also excluded patients who had undergone previous lacrimal surgeries and needed septoplasty or turbinectomy due to various nasal cavity abnormalities.
All surgeries were performed by a single experienced surgeon (SWY). Endonasal DCR was performed under general anesthesia using a nasal endoscope (Stryker endoscope 4.0 mm 0┬░). The nasal mucosa was injected with a 1 : 100,000 epinephrine solution. A mucoperiosteal incision was created in the projection of the lacrimal fossa to form a flap 10 mm in length. The nasal mucosa was removed with an elevator and Westcott scissors, and osteotomy was performed using a Kerrison punch. An intranasal bony ostium with a diameter of at least 10 mm was achieved. After tenting the lacrimal sac using a Bowman probe, the lacrimal sac was incised using a sickle knife. Bicanalicular lacrimal stents were tied with 6-0 prolene.
Three different anti-adhesion adjuvants were applied to the osteotomy site using a syringe in the nasal cavity after standard endonasal DCR: group A (71 eyes, Guardix-Sol 1.5 g), group B (89 eyes, HyFence 1.5 mL), and group C (38 eyes, Mediclore 1 cc). Hyaluronate and sodium carboxymethylcellulose (Guardix-Sol) was obtained from Hanmi Pharm (Seoul, Korea), and HyFence was obtained from CHA Bio & Diostech (Seoul, Korea). Mediclore was obtained from CGBio (Seongnam, Korea). Fig. 1A-1C shows the three different anti-adhesion adjuvants. Any intraoperative and postoperative complications were recorded.
Administration of oral antibiotics, nasal corticosteroids once daily, and eye drops containing antibiotics and steroids 4 times a day were prescribed to minimize granuloma formation and prevent stenosis postoperatively. The silicone tube was routinely removed 2 to 4 months postoperatively. Patients were evaluated based on lacrimal irrigation and by endoscopic observation of the nasal opening site. Patients were followed for at least 6 months, and they visited the clinic if ocular symptoms, such as epiphora or ocular discharge, recurred at any time.
In this study, success was defined as no complaint of tearing postoperatively. The results of the three groups were evaluated by asking patients about subjective symptoms and by performing lacrimal irrigation tests and endoscopic examinations. The main outcome measure was the success rate at follow-up at least 6 months after the operation.
Statistical analyses were performed using MedCalc (MedCalc Software Inc., Mariakerke, Belgium). Kruskal-Wallis analysis was used for comparisons of numerical variables; categorical proportions among the three groups were analyzed by Žć2 nonparametric analyses. All reported p-values are two-sided, and differences at a level of p < 0.05 were considered to indicate statistical significance.
Results
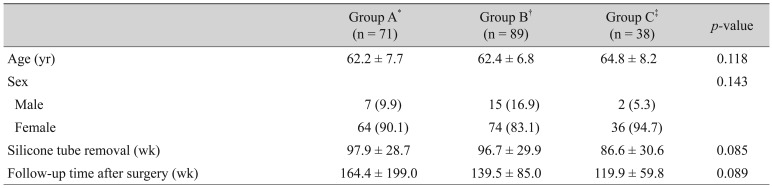
A total of 198 endonasal DCR procedures using anti-adhesion agents were performed in 151 patients. There were no statistically significant differences in age, sex, timing of tube removal, or follow-up period among the three groups (Table 1). At the last follow-up, success was achieved in 65, 82, and 35 cases in each group (91.5%, 92.1%, and 92.1%, respectively). There was no statistically significant difference in success rate among the three groups (p = 0.990). No major complications, including infection or uncontrolled epistaxis, were observed.
Discussion
Postoperative synechia formation is one of the common causes of endonasal DCR failure [5]. Therefore, Guardix-Sol has been used intraoperatively as an anti-adhesion adjuvant after endoscopic sinus surgery [6] and endonasal DCR [10]. In addition, biodegradable materials, including HA-based anti-adhesion agents and thermosensitive poloxamers (TPXs), have been used as barriers to prevent postoperative adhesion after endoscopic surgery [6,7,8,10,11]. However, the efficacies of HyFence and Mediclore in preventing adhesion after endonasal DCR surgery have not yet been elucidated. Therefore, we compared the efficacies of HyFence and Mediclore in preventing adhesion following endonasal DCR compared to Guardix-Sol.
HA is a ubiquitous polysaccharide component of the extracellular matrix. HA has been modified to improve its anti-adhesion property and sustainability due to the rapid biodegradability of natural HA [7,10,12]. Guardix-Sol, one of the HA-based anti-adhesion agents, is a liquid mixture of sodium hyaluronate and carboxymethylcellulose and has the advantages of improved sustainability and easier applicability than film-type barriers [6,13]. Therefore, Guardix-Sol is used intraoperatively as a biodegradable barrier during various surgeries including endonasal DCR [6,10,13]. However, sol-type barriers such as Guardix-Sol have a limitation for application in endonasal surgery as they can be easily washed away by gravity [6].
HyFence is also an HA-based anti-adhesion agent. The HA in HyFence is crosslinked with 1, 4-butandiol diglycidyl ether through a stabilization process to overcome the otherwise rapid biodegradability of natural HA. This cross-linked HA gel is comparatively less water-soluble and displays high viscoelasticity and stickiness [7,14]. Therefore, gel formulation of HA may be a good alternative to Guardix-Sol, which is a sol-type barrier.
When TPX is applied to the human body, the sol-type TPX is converted into a gel-type material due to its thermosensitive nature at body temperature [8]. Considering that the adhesion strength of an anti-adhesion agent that can withstand gravity once injected into a surgical area is an important factor, TPX may be advantageous as a biodegradable barrier. Hydrophilic polyethylene glycol components in poloxamers prevent adhesion with surrounding tissue [8,15]. TPX is used after endoscopic sinus surgery to prevent adhesion [8]. Mediclore, composed of poloxamer, gelatin, and chitosan, is a temperature-dependent sol-gel anti-adhesion product. The product is easily injectable at room temperature and is considered to have greater adhesion strength that can withstand gravity because of its sol-gel characteristics compared to Guardix-Sol, which is a sol-type barrier.
In our study, success was achieved in 65, 82, and 35 cases in each group (91.5%, 92.1%, and 92.1%, respectively). There were no major complications including infection or uncontrolled epistaxis. Therefore, our results suggest that HyFence and Mediclore can be safe alternatives to Guardix-Sol following endonasal DCR. Although there was no statistically significant difference in success rate among the three groups, the described anti-adhesion agents can be considered to be good alternatives for increasing the success rates of endonasal DCR in treating patients who possess the possibility of postoperative adhesion because of narrow nasal cavities or other nasal cavity abnormalities. Further studies will be needed to prove this.
This study has several limitations as it was a retrospective study. Moreover, the number of subjects in the Mediclore group was small at 38 cases. Another major limitation of this study was the relatively short follow-up period available to evaluate the effects of these materials in the long-term success of endonasal DCR. In addition, there was also no control group in which no adjuvant agents were used. Further study including a control group will therefore be needed to evaluate the effectiveness of the adjuvants. We also excluded patients who had previously undergone lacrimal surgeries and required septoplasty or turbinectomy due to various nasal cavity abnormalities because the number of these patients was too small. Therefore, further investigation will be needed to evaluate the effectiveness of various anti-adhesion agents in treating patients that are expected to have a poor prognosis.
In conclusion, HyFence and Mediclore constitute effective adjunctive modalities after endonasal DCR compared to Guardix-Sol. Therefore, these two agents can be safely used to increase the success rate of endonasal DCR in treating patients with the possibility of postoperative adhesion due to various abnormalities in the nasal cavity.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






