

Ocular disease caused by herpes simplex virus (HSV) infection occurs in 4.1 to 20.7 people per 100 thousand people every year, and the prevalence of HSV-induced ocular disease is 149 per 100 thousand people [1,2]. Eye disease caused by HSV infection mainly appears as blepharitis, conjunctivitis, and keratitis. Repeated recurrences can result in serious ocular diseases such as endothelial and stromal keratitis, which can induce permanent visual loss [3]. Although the administration of antiviral agents and corticosteroids is relatively effective in the acute inflammatory phase of keratitis, it does not prevent recurrence, which can lead to corneal opacity, corneal thinning, and neovascularization [4,5,6]. By contrast, the Herpetic Eye Disease Study (HEDS), which is an important prospective series of studies on the therapeutic and prophylactic effect of oral acyclovir in herpes simplex keratitis (HSK), has shown that prophylactic oral acyclovir administration reduces the frequency of stromal and epithelial keratitis recurrence [7,8,9]. However, a systematic review on the HEDS reported that the ability of various treatments to prevent HSK, including oral acyclovir, remains debatable [10].
Ascorbic acid is a co-factor for an enzyme that participates in collagen synthesis. It is a water-soluble antioxidant that can interact with reactive oxygen species and reduce the generation of radicals. Previously we reported systemic ascorbic acid administration reduced corneal opacity in infectious keratitis with a concomitant decrease of epithelial defect [11]. In addition, oral administration of ascorbic acid has been suggested to prevent HSV-1 reactivation under experimental environments [12,13].
The purpose of this study was to investigate the clinical characteristics and demographics of patients with HSK in South Korea and to determine whether oral acyclovir and oral ascorbic acid treatment can prevent HSK recurrence.
Materials and Methods
All consecutive patients with HSK who were referred to our tertiary eye clinic at Gyeongsang National University Hospital in Jinju, South Korea, between January 2010 and January 2015 were identified by a retrospective review of the medical records. All patients with HSK who were followed up for at least 6 months were included in the study. All patients initially presented in a local clinic and had been referred to our center. The hospital cornea specialist diagnosed patients with HSK based on patient history and the presence of typical clinical signs and symptoms. The complete ophthalmic examination included determining the best-corrected visual acuity (BCVA) and performing measurements, tonometry, slit-lamp anterior segment biomicroscopy, and fundus ophthalmoscopy. Complete ophthalmic examinations were also performed at each follow-up visit. Treatment was based on the clinical features and recurrences during follow-up. This study adhered to the Declaration of Helsinki, and approval for retrospective review of clinical records was obtained from the institutional review board of Gyeongsang National University Hospital (GNUH2018-07-020). According to the institutional review board standard operating procedures on retrospective single center clinical study, ethics committee of Gyeongsang National University Hospital ruled that subject consent was not required for this study. The clinical variables evaluated in the study were HSK subtype, the number and types of recurrences, the BCVA, the ocular complications during follow-up, and the treatment.
Clinical presentation and diagnosis
HSV ocular infections were diagnosed clinically on the basis of pathognomonic signs such as dendritic epithelial keratitis and iris atrophy. HSK was classified as epithelial keratitis, stromal keratitis, endotheliitis, and neurotrophic keratopathy subtypes. Epithelial keratitis was diagnosed when the lesion exhibited dendritic or geographic epithelial irregularity or ulceration. Stromal keratitis was diagnosed when necrotizing or immune stromal keratitis that had stromal nummular, patchy, sectorial infiltrate, or opacity was present. Endotheliitis was diagnosed when sectorial or nummular stromal edema that associated spatially with keratic precipitates was observed. Neurotrophic keratopathy was diagnosed when the patient had indolent interpalpebral epithelial irregularity or ulceration that lacked signs of acute infection. Patients with a history of herptic keratitis without any other cause, such as neurosurgical history or drug toxicity, were included in the neurotrophic keratopathy group. There were 7 cases in which two types were observed clinically at the same time, 4 cases were classified as endotheliitis in which mild stromal keratitis were combined with endotheliitis, 3 cases were classified as stromal keratitis in which mild epithelial keratitis was combined with stromal keratitis.
Treatment
All patients were treated according to the degree of intraocular inflammation, as determined by the location of the infection, the corneal or intraocular involvement, and the number of cells in the anterior chamber. Epithelial keratitis was treated with topical acyclovir and prophylactic antibiotic eye drops. Immune stromal keratitis was treated with topical steroids, and oral steroids were added in the presence of severe inflammation. Endotheliitis was treated with topical steroids, oral steroids, and oral acyclovir were added in the presence of severe inflammation or linear endotheliitis. Neurotrophic keratopathy was treated with nonpreserved artificial tears and prophylactic antibiotic eye drops. In severe cases of neurotrophic keratopathy in which the above regimen was inadequate, surgical treatment such as amniotic membrane transplantation was performed. After the acute phase, patients who experienced two or more HSK recurrences received prophylactic treatment with oral acyclovir (400 mg twice daily, total 800 mg), and treatment lasted at least one year. Oral ascorbic acid was administered to all patients except if they were pregnant or lactating; had a chronic systemic disease such as liver disease, renal disease, uncontrolled diabetes mellitus, or hypertension; had a history of renal calculi or gout; or had a history of allergic reaction to ascorbic acid. Each patient was given one 1,000 mg ascorbic acid tablet (Korea Eundan, Seoul, Korea) two times per day.
Statistical analysis
All statistical analyses were performed using IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ┬▒ standard deviation, and categorical variables were expressed as percentages. The distribution of the continuous variables was assessed using one-sample Kolmogorov-Smirnov tests. Groups were compared using the chi-squared test, the independent samples t-test, and the one-way analysis of variance test. Univariate and multivariate logistic regression analyses were used to identify risk factors for HSK recurrence. A p-value below 0.05 was considered as statistically significant.
Results
Demographic and main clinical characteristics
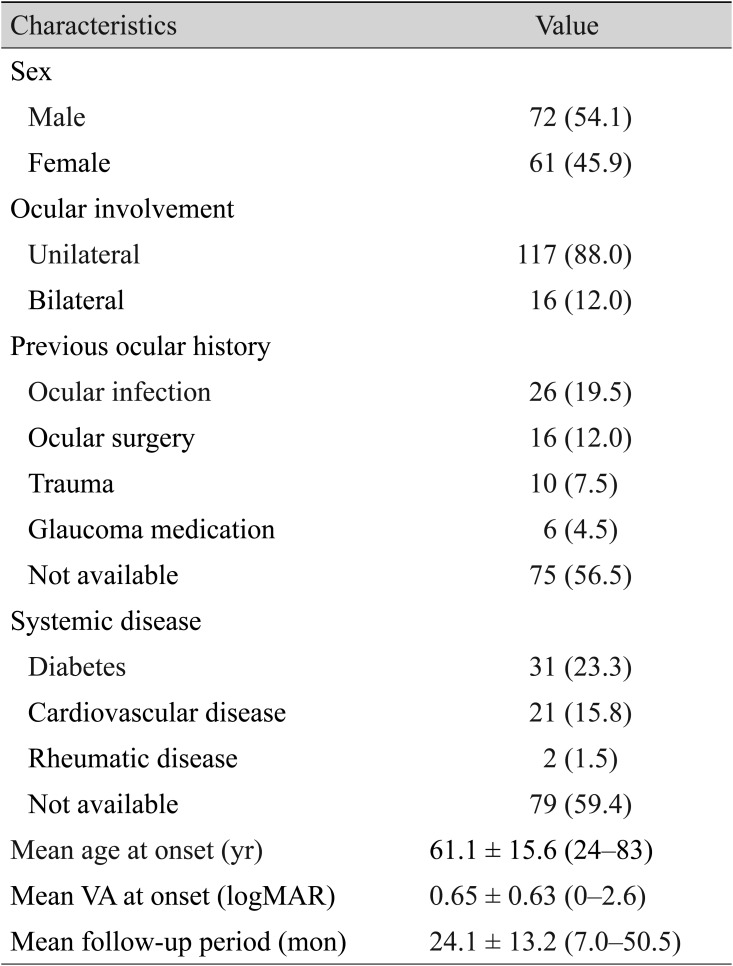
The general characteristics of all patients are summarized in Table 1. In total, 133 patients (72 male and 61 female) with 149 affected eyes were included in the study. The patients were followed for 24.1 ┬▒ 13.2 (range, 7 to 50.5) months on average. The mean age of HSK onset was 61.1 ┬▒ 15.6 (range, 24 to 83) years, and the mean BCVA at onset was 0.65 ┬▒ 0.63 (range, 0 to 2.6). Ocular involvement was unilateral in 117 (88%) cases and bilateral in 16 (12%). Twenty-six (19.5%) patients had a past ocular history of ocular infection such as blepharitis, infectious conjunctivitis, corneal ulcer, and endophthalmitis, while 31 (23.3%) patients had been diagnosed with diabetes at the time HSK was diagnosed.
Clinical features of patients with HSK subtypes
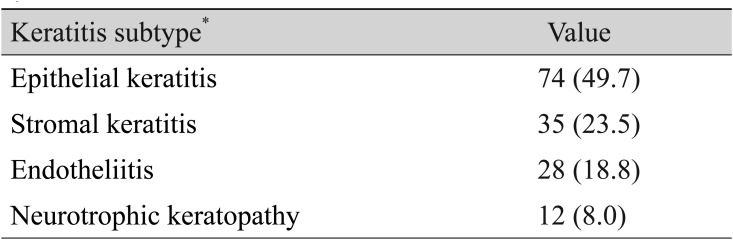
Table 2 shows the number of patients and eyes with the various HSK subtypes. Of the 149 affected eyes, 74 (49.7%) had epithelial keratitis, 35 (23.5%) had stromal keratitis, 28 (18.8%) had endotheliitis, and 12 (8.0%) had neurotrophic keratopathy.
Analysis of the BCVA at presentation and at the final visit for patients in each subtype group showed that stromal keratitis associated with the lowest BCVA at both time points. However, the subtypes did not differ significantly in terms of the BCVAs at either time point (Table 3).
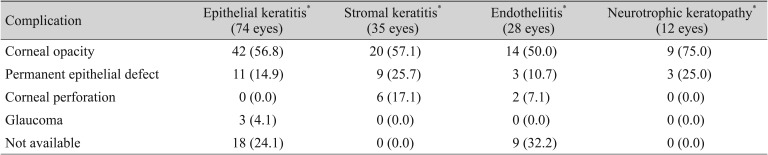
Table 4 shows the ocular complications that were encountered during follow-up in each HSK subtype group. Corneal opacity was the most frequently seen ocular complication in all four subtypes. Corneal perforation, which is a severe complication, occurred in six eyes with stromal keratitis and in two eyes with endotheliitis.
Recurrences
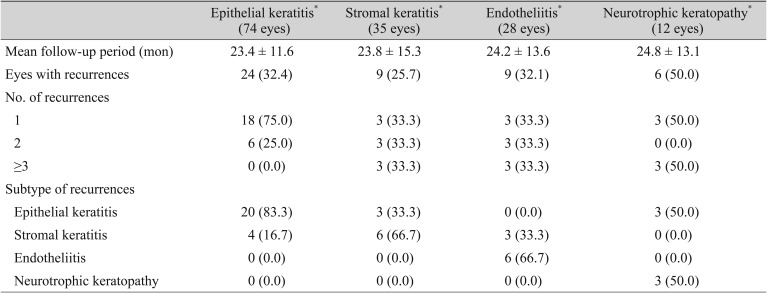
All patients were classified according to their follow-up duration, and the recurrence rate was higher with the longer follow-up duration: 16.7% (13 / 78) within 1 year, 25.9% (7 / 27) between 1 and 2 years, 53.8% (14 / 26) between 2 and 3 years, 77.8% (14 / 18) over 3 years. The numbers of HSK recurrences in the four HSK subtype groups during follow-up are shown in Table 5. The types of ocular disease in the recurrences are also shown. Overall, 48 of 149 eyes (32.2%) exhibited one or more recurrences during follow-up. There was no significant difference in the follow-up period between the HSK subtype groups (p = 0.983). The eyes that presented initially with neurotrophic keratopathy had the highest recurrence rate (6 of 12 eyes, 50.0%), followed by epithelial keratitis (24 of 74 eyes, 32.4%), endotheliitis (9 of 28 eyes, 32.1%), and stromal keratitis (9 of 35 eyes, 25.7%). The number of recurrences ranged from one to three; none of the eyes recurred more than three times. In the epithelial keratitis, stromal keratitis, and endotheliitis groups, the eye disease in the recurrence was mostly the same subtype as the eye disease in the first episode (83.3%, 66.7%, and 66.7%, respectively). However, in the six patients with neurotrophic keratopathy who exhibited recurrences, only three (50%) recurred as neurotrophic keratopathy (50%); the remaining three (50%) recurred as epithelial keratitis.
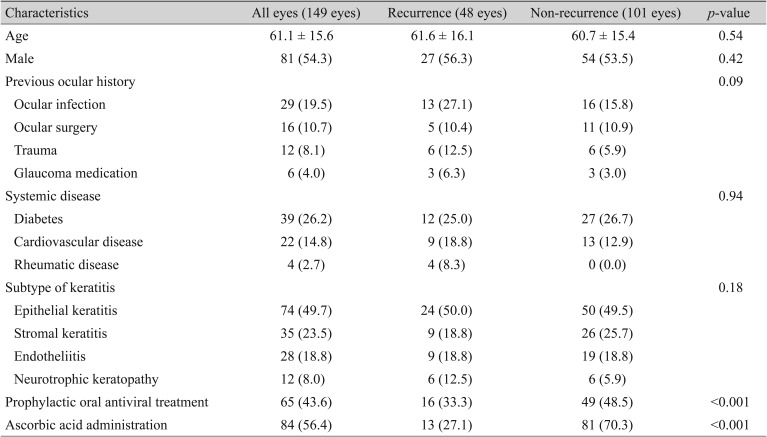
When the eyes with and without recurrence were compared, the two groups did not differ significantly in terms of age, sex, previous ocular history, systemic disease, or HSK subtype frequency. However, the recurrence rates were lower in prophylactic oral antiviral agent group (16 / 48 eyes, 33.3% vs. 49 / 101 eyes, 48.5%) and ascorbic acid treatment group (13 / 48 eyes, 27.1% vs. 81 / 101 eyes, 70.3%) compared to the groups without medications (Table 6). Univariate logistic regression analysis revealed that prophylactic oral antiviral agent significantly lowered the risk of recurrence (odds ratio, 0.51; 95% confidence interval, 0.12 to 0.51; p < 0.001). Oral ascorbic acid administration also significantly reduced the recurrence risk (odds ratio, 0.25; 95% confidence interval, 0.20 to 0.91; p = 0.04). In addition, multivariate logistic regression analysis showed that prophylactic oral antiviral agent and oral ascorbic acid administration significantly decreased the recurrence rate (odds ratio, 0.62, 0.30; 95% confidence intervals, 0.31 to 0.87, 0.13 to 0.69; respectively) (Table 7).
Discussion
HSK is a major cause of ocular morbidity worldwide. The overall incidence of HSK episodes is 31.5 per 100 thousand people-years, while the incidences of initial and recurrent cases are 13.2 and 18.3 per 100 thousand people-years [14]. Despite this, there are relatively few recent reports on the epidemiology and clinical manifestations of HSK in Asia. In the present study, we report the clinical characteristics and recurrence rates of eyes with HSK that were followed in our tertiary referral center in Jinju, South Korea. There was a preponderance of males (54.1%) in our study cohort. Similarly, previous reports have shown that in Korea, males are more commonly affected by HSK than females [6,15]. The mean age of HSK onset in our study was 61.1 years, which is higher than that reported previously in Korea (54.6 years) [15]. This may reflect the demographic characteristics of the population of the southern part of Korea, in which our center is located: the people in this region are older on average than the people in other parts of Korea.
The most common subtype of HSK in our cohort was epithelial keratitis (49.7%). Two large epidemiological studies in the United States of America and in France reported somewhat higher rates of epithelial keratitis (60% [2] and 66% [14], respectively). The next most frequent HSK subtype in our study was stromal keratitis (23.5%). The US and French studies reported similar frequencies [2,14]. It should be noted that the frequencies of subtypes recorded in the present study may reflect some inadvertent selection bias: although we included all consecutive patients with HSK in the study period, our center is a tertiary referral center. Such centers are more likely to receive patients with more severe symptoms and signs. Since most patients with epithelial keratitis have minimal or no symptoms, most would be treated by the local clinics rather than our hospital.
There were no significant differences between the subtype groups in the present study in terms of BCVA at diagnosis or at last follow-up. However, of all four subtype groups, the stromal keratitis group tended to have the lowest BCVAs at both time points. This pattern mirrors the pattern of HSK complications in our study: corneal opacity, which was the most common complication in our patients, was particularly frequent in the stromal keratitis group. This factor may account for the tendency towards a lower BCVA in the stromal keratitis group. The prevalence of cataracts as complication of herpetic keratitis was low in our cohort. By contrast, a retrospective study in a tertiary care facility in Italy found complicated cataracts rates of 27.5% [16]. Thus, the prevalence of complicated cataracts may be shaped by racial physical or anatomical characteristics. Further studies on this issue are warranted.
The recurrence rate in our cohort (32.2%) was similar to that reported by other epidemiological studies [7,9,17]. However, we noted that the stromal keratitis group had a lower recurrence rate than the epithelial keratitis or endotheliitis groups. By contrast, the HEDS suggested that patients with previous episodes of stromal keratitis (particularly those with numerous such episodes) were at greater risk of stromal keratitis recurrence [18]. To investigate this matter further, we examined the association between various factors and risk of recurrence by univariate analyses. Age and gender did not associate significantly with recurrent HSK risk. This was also observed by the HEDS [18]. We also did not find that past ocular history, systemic disease, or HSK subtype associated significantly with recurrence risk. However, we did find a significant association between prophylactic oral acyclovir treatment (400 mg two times daily) and a reduced risk of HSK recurrence. This is supported by the HEDS that showed that 400 mg of oral acyclovir twice daily for 1 year reduced the 1-year ocular HSV recurrence rate by approximately 45% [8]. Thus, the present study supported the notion that prophylactic oral acyclovir treatment lowers the risk of HSK recurrence.
In the present study, oral ascorbic acid treatment was associated with a reduced risk of HSK recurrence. To the best of our knowledge, the ability of this treatment to prevent HSK recurrence has not been reported previously. Supporting our finding is that some forms of ascorbic acid have antiviral properties: 2-O-glycoside of ascorbic acid displays marked antiviral properties against HSV-1, influenza, and poliovirus [19], while dehydro-ascorbic acid may affect HSV-1 multiplication after completion of viral DNA replication at the maturation stage [20]. Our previous study showed that the ascorbic acid concentration in the aqueous humor is increased by systemic ascorbic acid supplementation, and this increased ascorbic acid may have affected the recurrence of herpetic keratitis [21]. Such antiviral properties may explain why oral ascorbic acid treatment was found in the present study to associate with lower HSK recurrence rates.
Our study has some limitations. First, it was a retrospective study with a relatively short follow-up period. Second, the treatment of the patients was not dictated by standard guidelines; rather, the treatment decisions were made by multiple physicians on a case-by-case basis. This may have introduced selection bias in the study. Third, because the diagnosis was made based on clinical findings and past history, it is possible that a diagnostic error occurred. These limitations indicate the need for prospective randomized studies that assess the ability of oral ascorbic acid treatment to prevent HSK recurrences. Such studies are also needed to determine the most effective dose of ascorbic acid. Studies that measure the ascorbic acid concentrations in the cornea and anterior chamber of patients with HSK are also warranted.
In conclusion, the present retrospective study provides clinical information on the clinical characteristics and recurrence rates of HSK in a Korean referral center. To our knowledge, this is the first study to show that oral ascorbic acid treatment may prevent HSK recurrence. Although there are limitations with a retrospective study, this study demonstrates the potential of oral antiviral treatment and ascorbic acid administration to prevent the recurrence of HSK.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






