Macular Thickness in Moderate to Severe Amblyopia
Article information
Abstract
Purpose
To compare the macular retinal thickness of moderately to severely amblyopic eyes with non-amblyopic eyes as controls.
Methods
This case control study was conducted on 56 children aged 4 to 10 years old (64.3% female subjects). Twenty-eight children had unilateral amblyopia (28 amblyopic eyes as cases and 28 normal fellow eyes as internal controls) and 28 children had normal visual acuity in both eyes and were considered as external controls (n = 56 eyes). Among our cases, 14 had strabismic amblyopia and 14 had anisometropic amblyopia. Macular retinal thickness was measured using optical coherence tomography at the center and in 1-, 3-, and 6-mm rings.
Results
Best-corrected visual acuity of the amblyopic eyes was less than that of the internal and external controls, and the best-corrected visual acuity of their fellow eyes was also less than that of the external controls. Thickness of the central macula and a 1-mm ring area in the amblyopic eyes was higher than that of both internal and external controls. Difference of central macular thickness ≥20 µm between two eyes of the amblyopic children was significantly more than non-amblyopic subjects.
Conclusions
Based on the results of this study, the macular retinal thickness was significantly higher in moderate to severe amblyopic eyes compared to their fellow eyes and external controls. This might be due to macular developmental disorders in amblyopic eyes. Therefore, optical coherence tomography imaging is recommended if subtle macular abnormalities are suspected in moderate to severe amblyopic eyes.
Functional amblyopia is a unilateral or bilateral reduced best-corrected visual acuity (BCVA) with a prevalence of 2% to 5% according to various reports [123456]. Uncorrected refractive errors, ocular deviations and visual deprivation during childhood are known as amblyogenic factors [78]. In some amblyopic cases, there is no specific reason for reduced BCVA, named idiopathic amblyopia [1]. Different therapeutic approaches including prescribing appropriate glasses or contact lenses and patching and penalization of the dominant eye have been applied. The success rate of amblyopia therapy depends on the severity of reduced vision, type of refractive errors, ocular alignment, age of treatment, and the compliance of the child and his or her family [9]. According to the literature, successful amblyopia therapy was achieved only in about 50% of amblyopic cases [1]. Recently, subtle pathological variations in the macular area which are not noticeable in routine examination have been suggested as the cause of reduced vision in amblyopic cases who are not responsive to treatment [1].
Optical coherence tomography (OCT) is a non-invasive and non-contact type of fundus imaging with high repeatability and reliability that is not influenced by uncorrected refractive errors or illumination conditions [57]. Therefore, OCT has been described as a useful tool in presenting subtle macular pathologies in these cases [1234567]. Liu et al. [1] measured the average retinal thickness at about 130 ± 17.4, 153.8 ± 17.6, and 176.7 ± 14.8 µm at the center, fovea (1 mm) and macular areas (6 mm), respectively, in 7- to 14-year-old non-amblyopic Chinese children. According to the recent literature, increased retinal thickness at the macular area and decreased foveal depression were reported by OCT in amblyopic children [10]. This could be attributed to the lack of apoptosis of the ganglion cells, which normally occurs after birth [5]. Therefore, the foveal depression and its clinically bright reflex is reduced, but there was not consensus in all related studies [1234567]. In a meta-analysis by Li et al. [11] in 2015, 28 clinical trials were reviewed. They concluded that foveal minimum thickness, mean foveal thickness, mean macular thickness and peripapillary retinal nerve fiber layers were higher in amblyopic eyes compared to their fellow eyes. They also found no significant difference between anisometropic and strabismic amblyopic cases in this regard.
Furthermore, Kasem et al. [12] reported a higher thickness of central macular thickness, mean macular volume, and retinal nerve fiber layers in amblyopic eyes compared to their fellow eyes, and they found that axial length and age were independently correlated with central macular thickness. However, Chen et al. [13] did not find any difference between the foveal retinal thickness of amblyopic eyes and their controls. Their findings revealed higher thickness of the peripheral retina only in 2 to 4 quadrants as well as higher thickness of the nasal nerve fiber layer. They also concluded that amblyopia may induce diffuse variability in structure of the involved eyes, which requires further investigation.
Some authors believe that increased macular retinal thickness could be due to the high refractive errors (>±5.00 diopters [D]) or even artifacts [7]. In the previous study conducted by the same author, there was no significant difference between the amblyopic cases and their controls regarding macular retinal thickness, which could be due to the inclusion of a high percentage (86%) of mild amblyopic cases [14].
In the present study, we aimed to compare the macular retinal thickness of moderate to severe amblyopic eyes with non-amblyopic ones as their controls.
Materials and Methods
In this case-control study, 28 unilateral moderate to severe amblyopic cases (anisometropia [n = 14] and strabismus [n = 14]) with the age range of 4 to 10 years old were included. Their amblyopic eyes and their fellow eyes were considered as our cases and internal controls, respectively. In addition, 28 non-amblyopic children were enrolled as our external controls. First, cases were selected based on our inclusion criteria, then controls were included after matching for age, sex, anisometropia, and strabismus in the anisometropic and strabismic amblyopic groups, respectively.
All children with a history of developmental delay, prematurity (birth weight <1,500 g and gestational age less than 34 weeks) [15], congenital ocular anomalies, fundus lesions, previous ocular surgery, nystagmus, glaucoma, bilateral amblyopia, age over 10 years old, eccentric fixation, and high ametropia (>±5.00 D) were excluded from the study. All cases in this study were newly diagnosed and treated.
This study was approved by the ethics committee of Ophthalmic Research Center, Shahid Beheshti University of Medical Sciences (93-92322). The informed consent letter was signed by the parents of all participants.
Cyclorefraction was performed 45 minutes after instillation of cyclopentolate 1% and tropicamide 1% eye drops with an interval of 5 minutes. Anisometropia was considered as a spherical equivalent difference of at least 1.50 D between the two eyes. BCVA was assessed using the crowded Snellen E-chart (SIFI Diagnostic SPA, Treviso, Italy) at a distance of 6 m. BCVA in the range of 20 / 50 to 20 / 100 was considered as moderate amblyopia, and BCVA of less than 20 / 100 was defined as severe amblyopia [816]. Ocular motility was also evaluated in 9 different visual gazes by duction and version. Ocular misalignment was also measured at far (6 m) and near (33 cm) distances using the alternative prism cover test or the Krimsky method. Anterior and posterior segments were examined with a slit lamp and an indirect ophthalmoscope. In addition, stereopsis was assessed using the Titmus test.
The amblyopic cases were treated with appropriate glasses after cycloplegic refraction. Patching of the dominant eye for 4 hours per day in moderate and 6 hours per day in severe amblyopia for 1 to 3 months (at least 1 week for each year of age) were also ordered [16]. We measured the macular retinal thickness of both eyes with OCT (3D OCT-1000; Topcon, Tokyo, Japan) at the center and at 1-, 3-, and 6-mm rings in different segments (superior, inferior, nasal, and temporal). Differences of macular retinal thickness more than 20 µm between the two eyes was also considered clinically significant (about one tenth of central macular thickness). In the present study, the macular thickness of moderate to severe amblyopic eyes was compared with their internal and external controls.
To describe data, we used mean, standard deviation, median, and range. To compare the subject specific variables, we used Mann-Whitney, chi-square, and Kruskal-Wallis tests. To compare the eye-related variables and considering the probable correlation of the eyes, we used the generalized estimating equation. All statistical analysis performed by IBM SPSS ver. 23 (IBM Corp., Armonk, NY, USA). All tests were two sided and a p-value less than 0.05 was considered as statistically significant.
In the Whisker plot (Fig. 1, 2), the horizontal line in the middle of plot demonstrates the median of the values in each group. The box represents the interquartile range (from the first to third quartile) and the whiskers (errors) showed the possible range (minimum and maximum values).

Central retinal thickness (foveola) in (A) strabismic and (B) anisometropic amblyopic and control eyes.
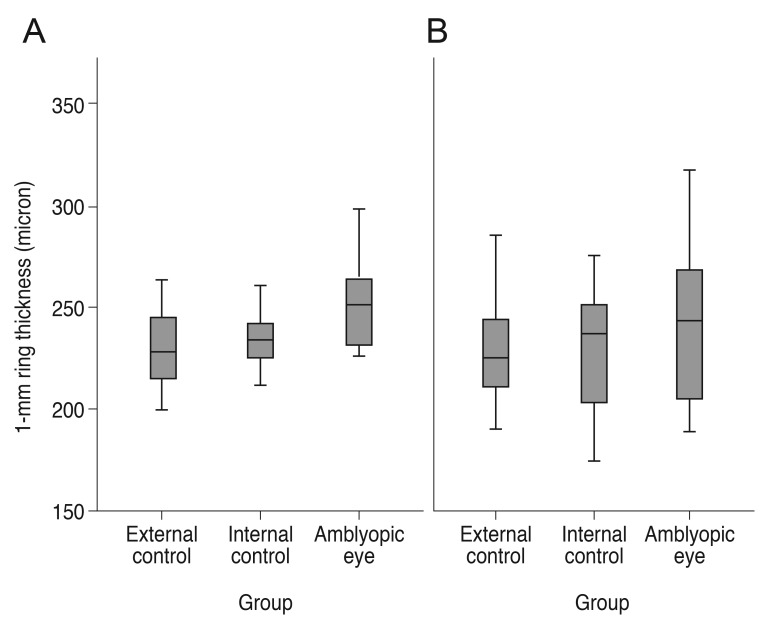
Retinal thickness at 1-mm ring (fovea) in (A) strabismic and (B) anisometropic amblyopic and control eyes.
Results
We included 56 children (n = 112 eyes) including 28 unilateral amblyopic and 28 non-amblyopic children with a mean age of 7.2 ± 2 years (range, 4 to 10 years).
As presented in the Table 1, there was no statistically significant difference between cases and controls regarding their baseline characteristics and the type of amblyopia.
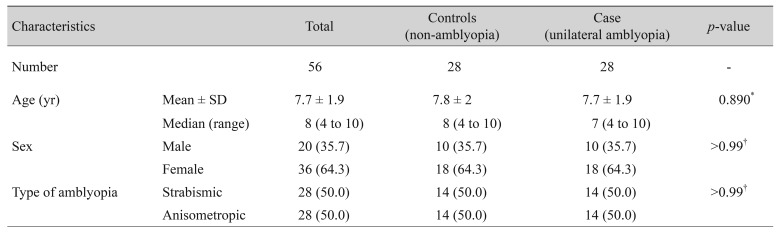
Characteristics of children in the case and control groups
The mean BCVA in the case group (amblyopic eyes) was 0.57±0.19 logarithm of the minimum angle of resolution (logMAR), which was significantly lower than that of the internal (0.03 ± 0.05 logMAR) and external (0.02 ± 0.06 logMAR) control groups (p < 0.001 for both). The mean BCVA of the internal controls was also less than that of the external control group (Table 2).
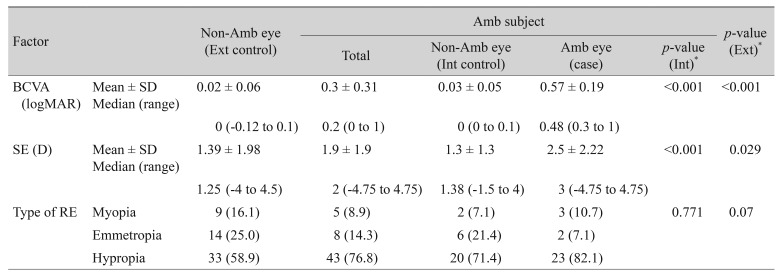
BCVA and refractive status of children in the case and control groups
The mean spherical equivalent of refractive errors was higher in the amblyopic eyes compared to the internal and external controls (p < 0.001 and p = 0.029) (Table 2), though there was no significant difference between amblyopic cases of anisometropic and strabismic groups regarding different types of refractive errors (Table 3).
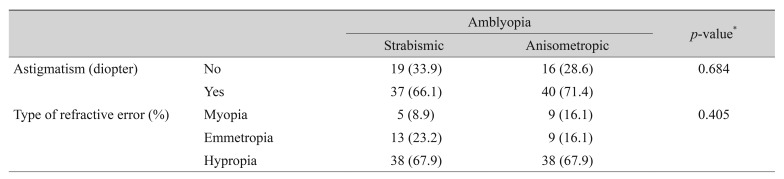
The percent of cases with different types of REs in different amblyopic cases
The mean macular retinal thickness of the amblyopic eyes at the central and foveal areas (1-mm ring) was higher than both internal and external controls, whereas this difference was not observed at the 3- and 6-mm rings (Table 4).
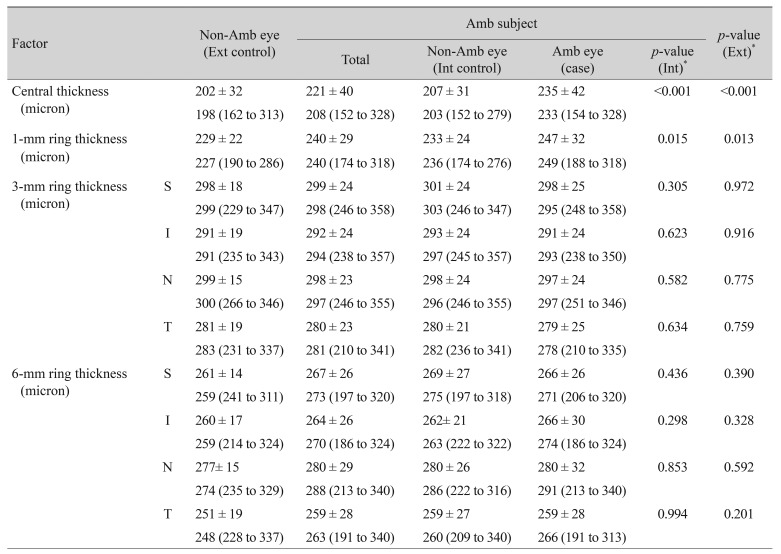
Retinal thickness of the case and control groups
In addition, a more clinically significant difference in central retinal thickness (≥20 µm) was observed between two eyes of amblyopic cases compared to non-amblyopic children (p = 0.013) (Table 5), while it was statistically borderline at the 1-mm ring (p = 0.055).
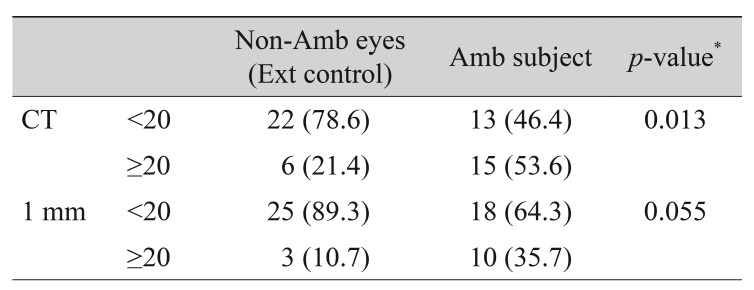
Difference of retinal thickness between two eyes from amblyopic subjects and their external controls
There was also higher retinal thickness at the center (275 ± 39 vs. 220 ± 33, p < 0.001) and the 1-mm ring (277 ± 27 vs. 235 ± 26, p < 0.001) in severely amblyopic eyes compared to moderately amblyopic eyes.
Among the strabismic amblyopic eyes, the macular retinal thickness at the central and foveal areas was higher than both control groups, whereas in anisometropic amblyopic eyes, the higher retinal thickness was only observed at the center of the macula (Fig. 1, 2). In addition, no significant difference in macular retinal thickness at the center (p = 0.945) and the 1-mm ring (p = 0.413) was observed between strabismic and anisometropic amblyopic eyes (Fig. 1, 2).
Discussion
In the present study, there was a significant difference in macular retinal thickness at the center and 1-mm ring area in the moderately to severely amblyopic eyes compared to the non-amblyopic controls (Table 4), although this difference was not found in the previous study conducted by the same author on mildly amblyopic children [14].
Furthermore, clinically significant differences of retinal thickness at center or at fovea in two eyes of the amblyopic children was higher than the non-amblyopic ones.
In a study by Altindag [10], macular thickness was significantly higher in strabismic amblyopic cases compared to the controls, similar to our present study. In addition, our findings were in line with a previous study [17] regarding higher central thickness in anisometropic amblyopic eyes. Liu et al. [1] measured a mean retinal thickness of 201.5 ± 17.9 and 176.7 ± 14.8 µm at the central and foveal areas in refractory amblyopic eyes, respectively, and they also found a significant difference when compared with normal Chinese children. This result was also observed in our study, with more average retinal thickness that could be due to the different races and measuring equipment. Furthermore, consideration of controls from another study does not seem to be logical, and it was better that both cases and controls were selected simultaneously from the same population.
Andalib et al. [18] also reported a significantly higher macular thickness in anisometropic amblyopic cases, though they did not find the same result in strabismic amblyopic cases. This inconsistency with our results could be due to their consideration of the whole macular retinal thickness instead of different ring areas. In addition, they compared their findings only with an internal control group (fellow eyes).
Aguirre et al. [19] found higher whole macular retinal thickness in mild and severe ametropic amblyopic eyes compared to controls. We believe that comparison of separate areas of macular thickness is a more logical method, as the center and 1-mm ring areas are more important than the 3- and 6-mm rings.
There was no significant difference in foveal retinal thickness between amblyopic and non-amblyopic eyes in a previous study [2]. The additional importance of subfoveal choroidal thickness measurement in the diagnosis of amblyopia has been investigated by different studies such as Kara et al. [20], Al-Haddad et al. [21], and Liu et al. [22], which all reported more sub-foveal choroidal thickness of amblyopic eyes compared to their fellow eyes and normal controls. They concluded that amblyopia may involve the subfoveal choroid even more than the retinal and peripapillary area.
Generally, increasing the retinal thickness of the macular area and decreasing foveal depression in amblyopic eyes could be attributed to the lack of apoptosis of ganglion cells, which normally occurs after birth [10]. Therefore, the foveal depression and its clinically bright reflex is reduced, but these inter pretations are controversial in the above-mentioned studies [1234567].
In the present study, we did not find a significant correlation between macular retinal thickness of the amblyopic children and different types of refractive errors (less than ±5.00 D). It is believed that myopia could interfere with normal macular development through the potential apoptosis of the ganglion cell, inner plexiform, and inner nuclear layers in the macular area; this could lead to macular dysplasia and probably failure of amblyopia therapy [23]. We did not study this, as we excluded children with high myopia from the present study.
The mean BCVA of the amblyopic eyes was less than that of both internal and external controls, and the BCVA of the internal controls was also less than that of the external control group (p < 0.001), as seen in our previous study [14]. This may be due to the existence of subtle variability in visual function in the healthy eye of unilateral amblyopic children. It is unclear whether fellow eyes of unilateral amblyopic children are thoroughly healthy, even with a BCVA of 20 / 20 to 20 / 30.
It should be noted that consideration of non-amblyopic children as the external control group is necessary in these types of investigations, with regard to the above-mentioned points.
One of the limitation of this study was the lack of refractive error matching between cases and controls, although we excluded children with a refractive error of more than ±5.00 D.
Based on the results of this study, macular retinal thickness was significantly higher in moderate to severe amblyopic eyes compared to their fellow non-amblyopic eyes and external normal controls. This may be due to macular developmental disorders in amblyopic eyes. Therefore, OCT imaging is recommended if macular abnormalities are suspected in moderate to severe amblyopic eyes.
Acknowledgements
The authors would like to thank all the children and their families who participated in this study.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.