

Three-dimensional (3D) displays, including 3D televisions (TVs) and 3D computers, are now available for home use due to progress in the 3D industry. Consequently, one can be exposed to 3D images at any time and for any duration. It has been documented that 3D images induce more ocular and systemic fatigue than 2D images, which is termed 3D asthenopia [1,2,3,4,5]. Moreover, the ocular and systemic effects of watching 3D images are not fully understood, and safe guidelines for 3D viewing have not yet been established. Therefore, any potential effects of exposure to 3D for a long duration of time, especially in children who are visually immature and also more interested in watching 3D images than adults, should be investigated to establish safe guidelines.
Myopia has a high prevalence in Asia; it is a leading public health problem with an incidence of up to 96.5% [6,7,8,9]. There have been numerous studies on the mechanism of myopia, and vigorous efforts have been made to reduce the development of myopia or to slow its progression [10,11,12,13,14,15,16,17,18,19]. Near work is a well-established environmental factor related to the development and progression of myopia [11,15,20]. Near work induces accommodation; after prolonged accommodation, transient myopic shift can be observed even after cessation of near work. This near work-induced transient myopia (NITM) is thought to be a possible environmental myopigenic factor [11,15]. Myopes are known to be more susceptible to NITM, and the severity of NITM is related to the amount and duration of accommodation. However, watching 3D images requires more accommodation than 2D viewing [21,22]. The 3D images with crossed disparity can induce fusional convergence and subsequent accommodation, which is unnecessary because the distance between the eyes and the screen does not change [23]. This accommodation-vergence conflict has been suggested as a cause of 3D asthenopia [3,4]. If unnecessary accommodation induces more transient myopic shift while watching 3D, it could be related to the development and progression of permanent myopia. In our previous study, we reported that watching 3D images on a computer monitor at a viewing distance of 50 to 70 cm induced a transient myopic shift more often than watching 2D content and suggested the possibility that 3D on a computer monitor might have a greater effect on myopia than 2D images [22]. However, the myopic shift after watching a 3D TV from a different viewing distance has not been evaluated but will be necessary to establish safe guidelines for watching a 3D TV.
The present study assessed the safety of watching 3D TV in regards to refractive errors by investigating the following questions: 1) Are there any refractive changes, such as transient myopic shift, after watching 3D TV? 2) Do myopes show a greater myopic shift? 3) In the participants who exhibited myopic shift, does the change of refractive error persist after a 10-minute rest?
Materials and Methods
The study protocol was reviewed and approved by the Korea University Anam Hospital Institutional Review Board and adhered to the tenets of the Declaration of Helsinki. Healthy volunteers between 6 to 12 years of age were recruited for this study. Informed consent was obtained from the parents of all participants. Before enrollment, prospective participants were given manifest refraction, slit lamp examination, fundus evaluation with fundus camera, alternate prism-cover test, and near stereopsis test with the Stereo Fly Stereotest (Stereo Optical Co., Chicago, IL, USA). The volunteers with strabismus, a best-corrected Snellen visual acuity less than 20 / 20, near stereoacuity worse than 60 seconds of arc, anisometropia more than 2.00 diopters (D), or any structural abnormalities in the cornea, lens, retina, or optic nerve were excluded from this study.
The 3D video was shown for 50 minutes on a 3D high-definition (HD) TV (UN55C7000WF; Samsung Electronics, Seoul, Korea), with a screen measuring 139 cm diagonally and while the participants wore liquid-crystal shutter glasses. The illuminance of the room was 5 lux, and the viewing distance was 2.8 meters. The viewing distance and duration were set according to the recommendations of the TV manufacturer and the International Telecommunication Union (2.2 meters or more for a 55-inch HDTV).
The 3D contents used in this study were produced by the national broadcasting system of Korea using a true 3D shooting technique for 3D test-run broadcasts; the image disparity ranged from -1 to 1 degree, and the reference depth was zero screen disparity.
The refractive error was obtained objectively with an autorefractor (RK-F1; Canon, Tokyo, Japan) before and immediately after watching 3D TV. It was rechecked after a 10-minute rest. At each time point, we repeated the measurement of refractive errors until we obtained the same value three consecutive times for each participant. The repeatability of the autorefractor was assessed using a coefficient of variation (0.64%), and it was highly reliable, as we reported in our previous study [22]. We used a spherical equivalent (sphere + 1/2 cylinder) of the right eye in this study. The refractive errors before and after watching 3D TV were compared. The participants with a spherical equivalent of baseline refractive error that was more than -0.75 D were included in the myopia group, and the other participants were placed in the non-myopia group [9]. The amount of refractive change after watching 3D TV was compared between the two groups. The refractive changes of the children who showed myopic shift at any amount were compared between each time point to determine whether the myopic shift persisted after a 10-minute rest.
The refractive errors showed a deviation from the standard distribution in the Shapiro-Wilk test. Therefore, we used non-parametric analysis in this study. The refractive errors before and after watching 3D TV were compared using the Wilcoxon signed-rank test. The amount of refractive change between the myopia and non-myopia group were compared using the Mann-Whitney U-test. A p-value for multiple comparison was adjusted with the Bonferroni correction.
Results
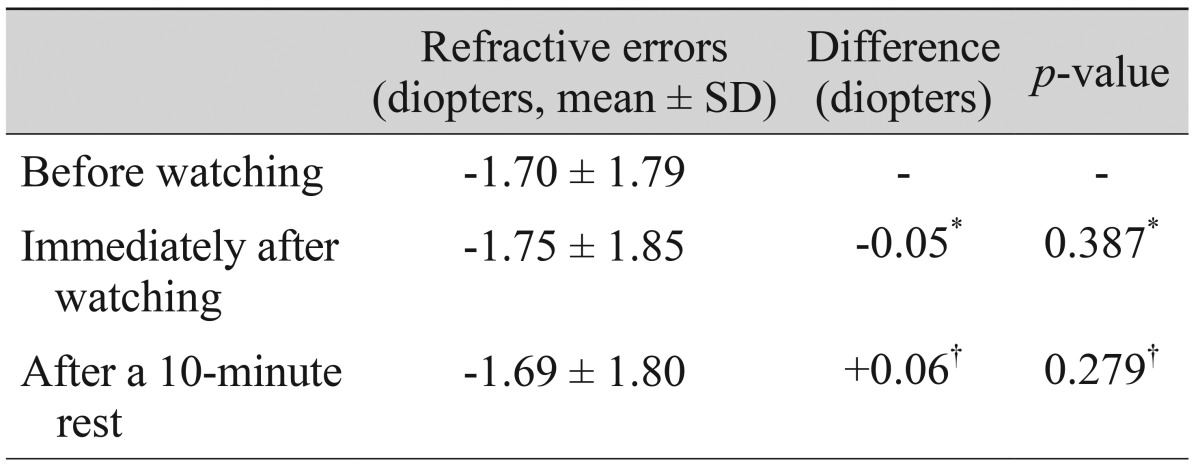
The mean age of the participants was 9.23 ± 1.75 years, and 29 were female (48.3%). The mean refractive error before watching 3D TV was -1.70 ± 1.79 (-5.50 to +1.25) D, and the refractive errors before and after watching 3D TV are shown in Table 1. There was no statistically significant difference between each time point.
The myopia group consisted of 34 children (56.7%). Table 2 shows the comparison in the change of refractive error between the myopia and the non-myopia group. The refractive errors did not change significantly in either group. The mean change of refractive error immediately after watching 3D TV was also not different between the two groups (p = 0.541).
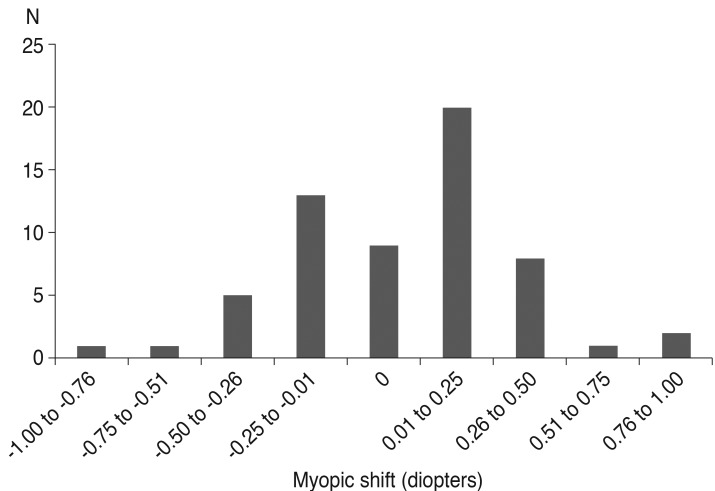
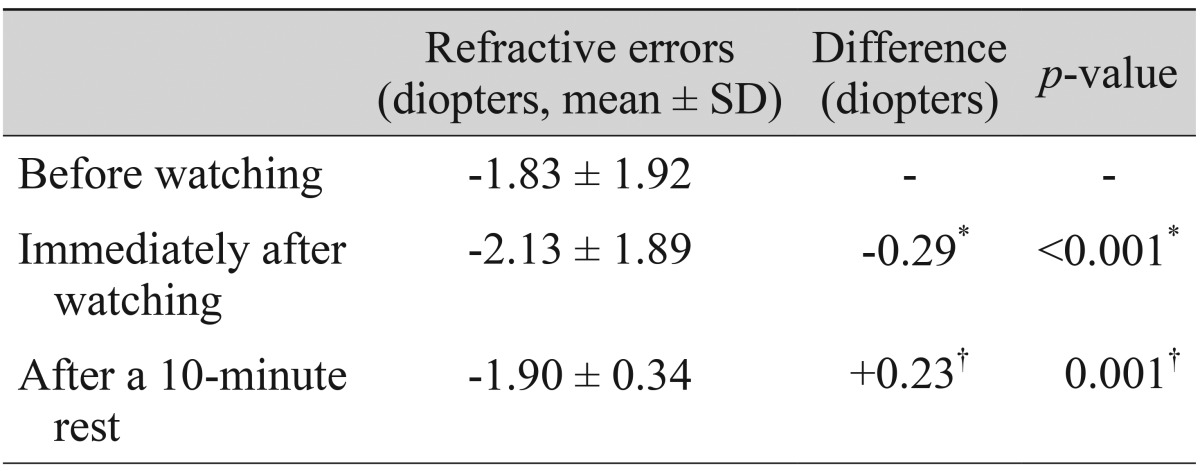
The distribution of refractive change before and immediately after watching 3D TV is shown in Fig. 1. The myopic shift was observed in 31 participants. The refractive error before watching 3D TV in these children (-1.83 ± 1.92 D) was not different from that in the others who did not show any myopic shift (-1.53 ± 1.68 D, p = 0.636). The age of the participants was also not different (p = 0.994). The refractive error significantly changed immediately upon watching 3D TV (p < 0.001) in the children with myopic shift, and the mean amount of myopic shift was 0.29 ± 0.23 (0.13-1.00) D (Table 3). However, these myopic shifts resolved after a 10-minute rest; therefore, the refractive error prior to watching 3D TV and after a 10-minute rest were not significantly different (p = 0.122).
Discussion
Our first question was in regards to the presence of refractive changes after watching 3D TV. The results showed that the mean refractive errors did not change after viewing 3D TV. In our previous study, we reported that watching 3D images induced a transient myopia that could be related to the development and progression of permanent myopia [11,15,19,24]. The differences between the previous and the current study were the viewing distance, duration and 3D content. In the previous study, the participants watched a 3D movie for 3 hours. The viewing distance was 50 to 70 cm. In the current study, a 3D movie was shown for 50 minutes with a viewing distance of 2.8 meters. The shorter duration of watching TV at a longer viewing distance might induce fewer changes of refractive errors. The image disparity of the 3D movie in this study was controlled to be -1 to 1 degree, which is known to be a zone of comfortable viewing of 3D, while that in the previous study was not controlled [4]. The shorter duration of watching a 3D movie with proper disparity at a longer distance might explain why the mean refractive errors did not change in the current study.
Our second question was about the difference of refractive response between myopes and non-myopic participants. Individuals with myopia are reported to be more susceptible to NITM [11,25]. Therefore, we compared the refractive change between the participants with myopia worse than -0.75 D (myopia group) and the other participants (non-myopia group). The myopia group contained 56.7% of the children in our study. The prevalence of myopia, defined as a refractive error worse than -0.75 D, was reported to be 50.0% of 1,560 participants from 5 to 11 years and 78.8% of 1,429 participants from 12 to 18 years in Korea [9]. The age group of our study was 6 to 12 years, so our prevalence of myopia was consistent with that study. The results of the current study revealed that myopes did not show more NITM than the non-myopia group. In most studies on NITM, the working distance was 20 to 40 cm [11,15,25]. Watching a 3D TV for 50 minutes at 2.8 meters did not influence the refractive error of myopic participants.
The third question was about the persistency of myopic shift, if present. In our study, 31 children experienced some type of myopic shift. Vasudevan and Ciuffreda [25] reported that NITM shows additivity, and they suggested that residual NITM might contribute to the progression of permanent myopia. In the current study, the mean refractive error of participants with myopic shift returned to baseline after a 10-minute rest without any residual NITM.
There are several limitations to this study. First, the number of enrolled participants was small. As a result, the lack of a statistical difference between the refractive errors before and after watching 3D TV does not prove that these refractive errors were the same, especially in a small sample size. A larger number of participants should be recruited to determine for certain that watching 3D TV from a safe distance does not induce transient myopia. The second limitation was that there was no 2D watching condition to serve as a control. However, the refractive error did not change after watching 3D TV, so we do not believe that a 2D control would be essential to assess the safety of watching 3D TV. This study's third limitation was that the viewing distance and duration were not varied. We had to employ a presumably safe viewing distance and duration because this study was intended to verify the safety of 3D TV watching in school-aged children. It would have been unethical to include a condition that involved an unsafe distance or duration. However, a variable viewing distance and watching time may have induced different results. The fourth limitation was that this study included no children with high myopia worse than -6.00 D. Although participants with mild to moderate myopia showed no significant myopic shift in this study, the response of refractive error in those with high myopia after watching 3D TV should still be evaluated. Further studies including a larger number of patients with a wider range of baseline refractive errors as well as with variable viewing times and distances will be necessary.
In conclusion, 50 minutes of watching a 3D TV with properly produced content at 2.8 meters did not induce transient myopic shift significantly in either myopic or non-myopic participants in this study. Those who showed myopic shift after watching a 3D TV recovered after a 10-minute rest. Therefore, it is recommended to view 3D contents for an appropriate duration and to include an intermission; in addition, at least 2.8 meters of viewing distance are recommended to watch 3D TV safely.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






