Accommodative Esotropia Who Needs Spectacles for Good Ocular Alignment after Refractive Shift below +2.00 Diopters
Article information
Abstract
Purpose
The aim of this study is to investigate the clinical characteristics of patients diagnosed with refractive accommodative esotropia (RAE) whose refractive errors were gradually reduced to below +2.00 diopters (D) during follow-up but use of spectacles was still required for maintenance of good ocular alignment.
Methods
We conducted a retrospective review of the medical records of patients diagnosed with RAE from 1995 to 2011. Patients were divided into 2 groups according to their ocular alignment at the last visit. Inclusion criteria were hyperopia ≥+2.00 D detected with cycloplegic refraction at the initial visit, which then became mild hyperopia (<+2.00 D) or myopia during follow-up, with more than 5 years of follow-up.
Results
A total of 92 patients met the inclusion criteria. Twenty-six patients showed persistent esotropia (≥10 prism diopters [PD]) without spectacles (group A) and 66 patients showed good ocular alignment (<10 PD) without spectacles (group B) at the last visit. No statistically significant differences in the spherical equivalent of the refractive errors at the initial and last visit were observed between the two groups. A significantly lower number of positive responses on the Lang I stereotest was observed in group A (n = 1, 3.8%) compared to group B (n = 22, 33.3%) (p = 0.003). There were increasing trends toward group A with worsening stereoacuity measured by the Stereo Fly Stereotest between the two groups (p = 0.016, linear by linear association). The results of the Lang I test, Stereo Fly Stereotest, and duration between the onset of esotropia and prescribing spectacles showed a significant association with the discontinuation of spectacles in the univariate logistic analysis.
Conclusions
Stereoacuity showed more significant associations than refractive errors in RAE with refractive error <+2.00 D but still required spectacles for maintenance of good ocular alignment. The prompt treatment of accommodative esotropia at the onset of esotropia is important for the discontinuation of spectacles.
Refractive accommodative esotropia (RAE) is one of the most common types of childhood strabismus associated with varying degrees of hyperopia [1,2,3,4]. The deviation is the result of an abnormal activation of the accommodation reflex required to overcome blurring caused by uncorrected hyperopia [4,5]; therefore, prescribing spectacles for correction of hyperopia has been a main treatment option for patients with RAE [1,5,6,7,8]. During the follow-up, most of the RAE patients experience a refractive shift toward decreasing hyperopia, even myopia [4,9,10,11]. Therefore, it is assumed that with the weakening of their hyperopia, patients with RAE would be spectacles-free. However, not all of the RAE patients who show a refractive shift toward decreasing hyperopia can discontinue wearing spectacles [4,6,12]. In clinical experience, some RAE patients can discontinue use of spectacles as they become less hyperopic during follow-up. However, others continuously require spectacles for maintenance of good ocular alignment, although they become mildly hyperopic or even myopic.
The purpose of this study was to assess the clinical characteristics and associated factors of patients with RAE whose refractive errors were gradually reduced to <+2.00 diopters (D) during follow-up but still required spectacles for maintenance of good ocular alignment.
Materials and Methods
Patient selection criteria
We retrospectively reviewed the medical records of patients with RAE who were diagnosed between January 1995 and December 2007 at Yeungnam University Hospital. Approval to conduct this study was obtained from the institutional review board of Yeungnam University Hospital. Diagnosis and follow-up were performed by a single strabismologist (MMK). Patients who met the following criteria were included in the study: RAE patients who had hyperopia ≥+2.00 D detected with cycloplegic refraction at the initial visit, but became mildly hyperopic (<+2.00 D) or myopic during follow-up, with at least 5 years of regular follow-up. Patients were divided into 2 groups according to their ocular alignment at the last follow-up, as follows: 1) RAE who showed a persistent esotropia (≥10 prism diopters [PD]) without spectacles (group A) and 2) RAE who showed a good ocular alignment (<10 PD) without spectacles (group B).
Patients with any other type of strabismus such as inferior oblique muscle overaction, dissociated vertical deviation or nystagmus were excluded from this study. Patients who had undergone previous extraocular muscle or intraocular surgery, or those with any neurologic impairment or deteriorating RAE were also excluded.
Patient evaluation
At the initial visit, all patients underwent a full ophthalmologic examination, including a visual acuity testing, ocular alignment status, slit-lamp biomicroscopy, cycloplegic refraction, fundus examination, and stereoacuity test. The onset of deviation was determined by a family member's description or old photographs, if necessary. Refractive errors were determined using retinoscopy under cycloplegia with 1% atropine instilled twice per day for 5 days [13]. Fundus examination was performed after the cycloplegic refraction test in all cases. Patients were initially prescribed a full hyperopic correction on the basis of their cycloplegic refraction. When esodeviation was not controlled with current spectacles, cycloplegic refraction was repeated. If additional uncorrected hyperopia was noted, the spectacles correction was changed. Ocular alignment with and without spectacles was measured by alternate prism cover testing at 6 m fixation and 33 cm fixation in every patient. Best-corrected visual acuity was measured when possible. Amblyopia was defined as an interocular difference in visual acuity of two lines or more. If amblyopia was found, the occlusion therapy was performed to treat amblyopia as soon as the effects of the corrective lenses were established. Stereoacuity was measured using the Lang I stereotest (Lang-Stereotest AG, Küsnacht, Switzerland) and the Stereo Fly Stereotest (Stereo Optical Co., Chicago, IL, USA) when the patient was able to cooperate and complete the test. The initial follow-up was performed at 3 months and the regular follow-up was generally performed every 6 months after ocular alignment became stable with no amblyopia. Weaning off the spectacles was considered in 8-year-old patients after their visual acuity and ocular alignment became stabilized. Weaning was accomplished by a gradual decrease of hyperopic correction, usually in 0.50 D increments on the basis of measured refractive errors at each visit.
Statistical analysis
Continuous data are presented as a mean with the standard deviation, and categorical data are presented as counts and percentages. Comparisons for continuous variables between 2 groups were performed using an independent t-test. The chi-square method (or Fisher exact test) was used to test the significance of differences between proportions and categorical variables. Linear by linear analysis was employed in order to identify the trends between stereoacuity and the discontinuation of spectacles. Univariate and multivariate logistic regression analyses were performed for the evaluation of associated factors with the discontinuation of spectacles. SPSS ver. 20.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analyses. A p-value <0.05 was regarded as statistically significant.
Results
Demographic and clinical characteristics between the two groups
A total of 92 patients met the inclusion criteria for this study. Of these 92 RAE patients, 26 were included in group A and 66 were included in group B. The demographics and clinical characteristics of these patients by group are shown in Table 1. Ten patients in group A (10 / 26, 38.5%) and 28 patients in group B (28 / 66, 42.4%) were not able to complete a visual acuity test at the initial visit because of a poor understanding of the test. During follow-up, 15 patients in group A (15 / 26, 57.5%) and 32 patients in group B (32 / 66, 48.5%) needed an occlusion therapy for treatment of amblyopia. One patient in group A (1 / 26, 3.8%) and 6 patients in group B (6 / 66, 9.1%) had amblyopia at the last visit (p = 0.67).
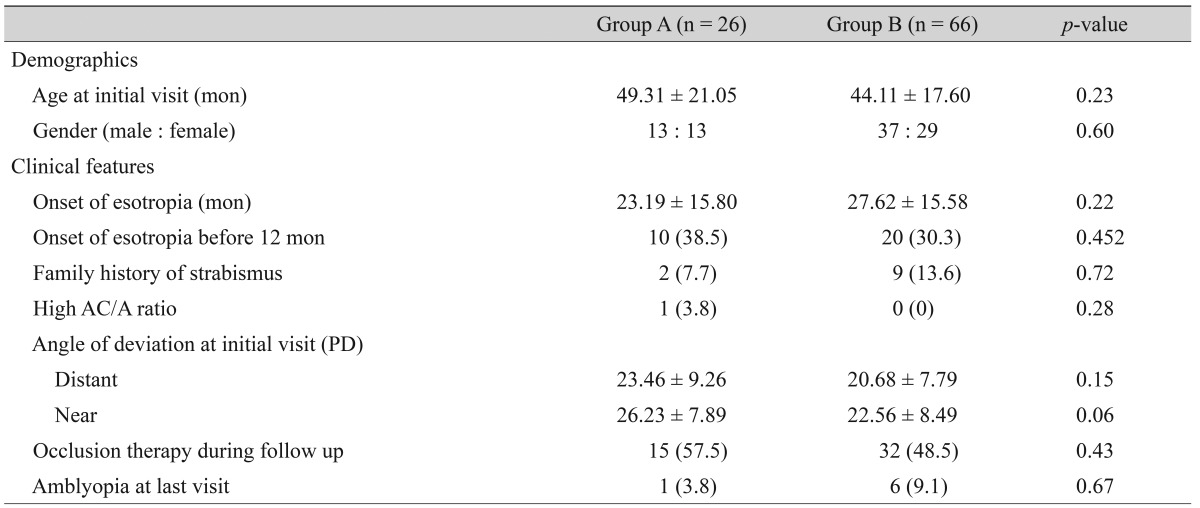
Comparison of the demographic and clinical characteristics of group A and B
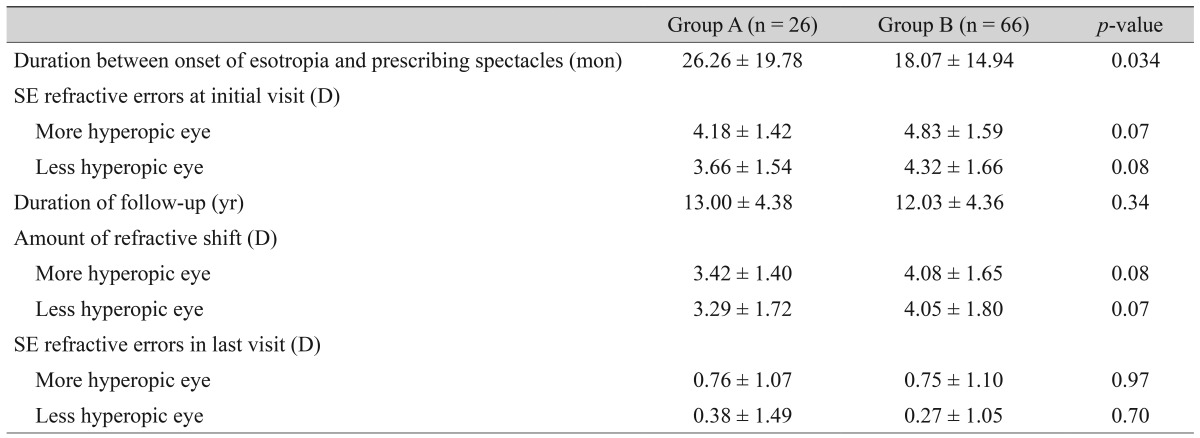
Differences in spherical equivalent refractive errors between two groups
Spherical equivalent (SE) refractive errors at the initial visit in groups A and B were 4.18 ± 1.42 D and 4.83 ± 1.59 D in the more hyperopic eye and 3.66 ± 1.54 D and 4.32 ± 1.66 D in the less hyperopic eye, respectively (Table 2). Among the variables, there was a statistically significant difference in the duration between the onset of esotropia and prescribing spectacles between the two groups (p = 0.034).
Comparison of the refractive errors of group A and B
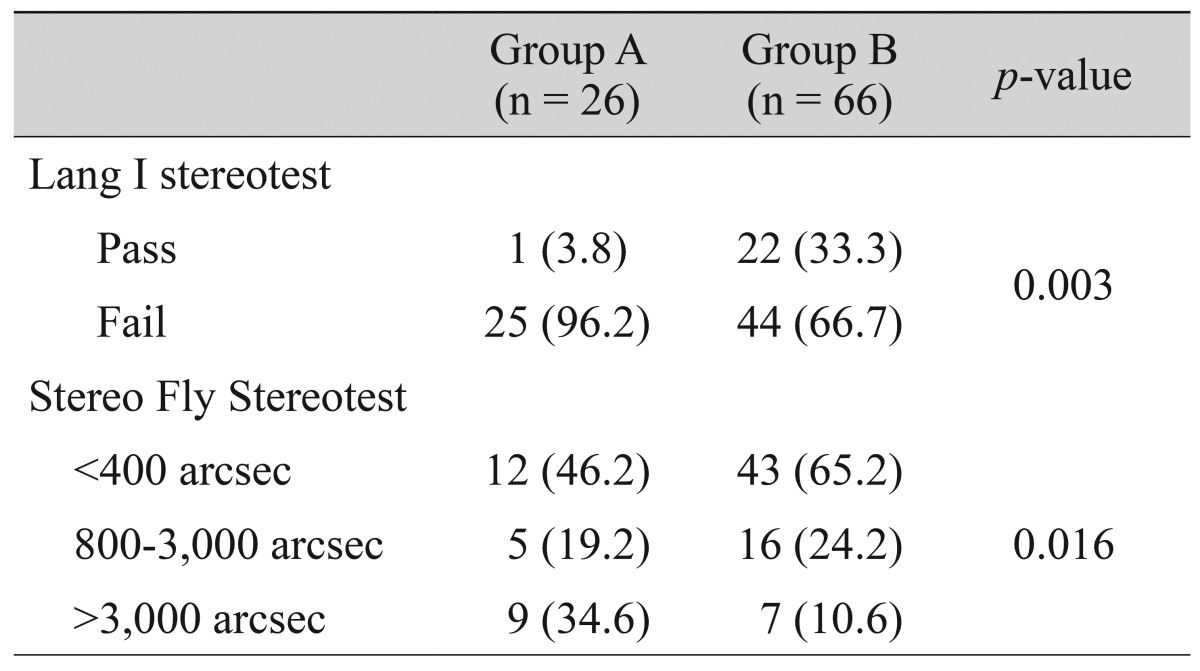
Differences in stereoacuity between the two groups
In the stereoacuity test, only one patient in group A (1 / 26, 3.8%) passed the Lang I stereotest compared to 22 in group B (22 / 66, 33.3%); this result showed statistical differences between the two groups (p = 0.003) (Table 3). To appreciate the trend between spectacles discontinuation and stereoacuity using linear by linear analysis, the results of the Stereo Fly Stereotest were stratified according to the degree of stereoacuity (<400 second of arc [arcsec], 800 to 3,000 arcsec and >3,000 arcsec). There were increasing trends toward group A with a worsening degree of stereoacuity measured by the Stereo Fly Stereotest, between the two groups (p = 0.016, linear by linear association).
Comparison of the stereoacuity of group A and B
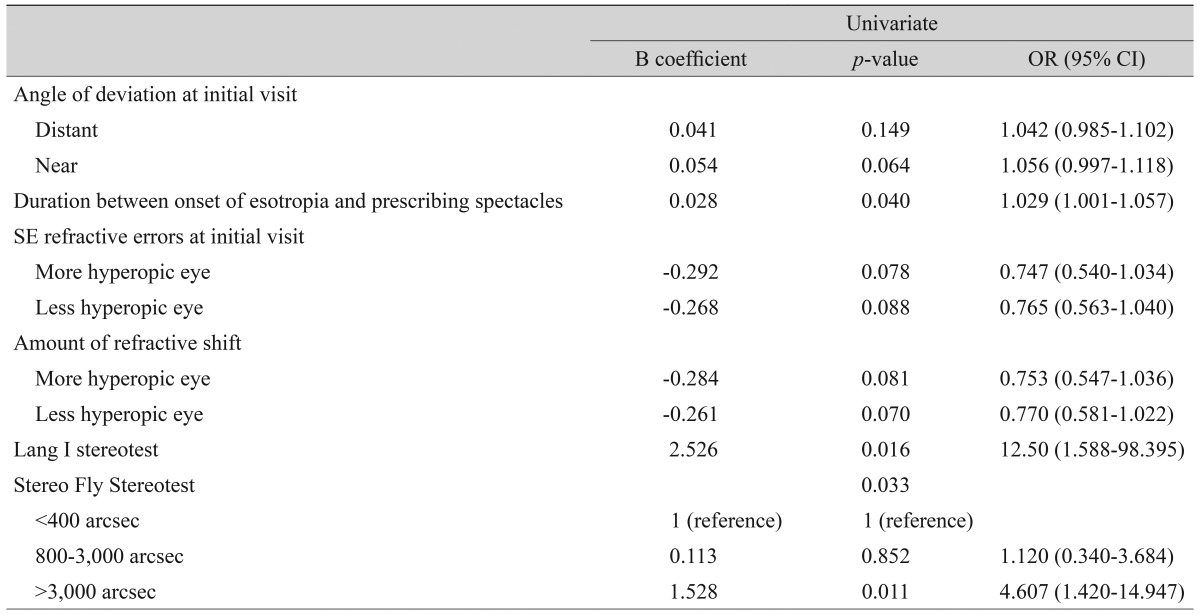
Factors associated with the discontinuation of spectacles using logistic regression analysis
The association between the discontinuation of spectacles and clinical characteristics was examined using both univariate and multivariate logistic regression analyses. All of the variables shown in Tables 1, 2 and 3 were first tested by univariate analysis; variables with p < 0.2 in univariate analysis are shown in Table 4. The duration between the onset of esotropia and prescribing spectacles, results of the Lang I stereotest and Stereo Fly Stereotest showed a significant effect on discontinuation of spectacles among variables (p < 0.05). Filtered variables with p < 0.2 in univariate analysis were further evaluated to identify their association with the discontinuation of spectacles using multivariate analysis. In the entry mode of the multivariate analysis, the result of the Lang I stereotest showed the strongest association with the discontinuation of spectacles (p = 0.039).
Results of univariate logistic regression analysis for the discontinuation of spectacles
Discussion
During follow-up for RAE, we are often asked by parents or patients whether or when the patient could be spectacles-free. Hyperopic refractive errors of RAE in patients usually decrease from the amount at the initial visit during follow-up. Therefore, it could be expected that RAE patients would discontinue use of spectacles. For the RAE patients who have gradually become mildly hyperopic from high hyperopia during follow-up and have hoped to be without spectacles, discontinuation of spectacles use might be considered the goal of treatment. However, not all of the RAE patients who have experienced a refractive shift toward mild hyperopia are able to discontinue use of spectacles. In our previous study, mild hyperopia (+2.00 D or less) can cause RAE, so we recommend the correction of hyperopia [14]. However, some patients showed good ocular alignment without spectacles as their refractive errors became mildly hyperopic during follow-up. For patients with RAE who became less hyperopic but required continuous use of spectacles for good ocular alignment, this result might be disappointing. These clinical experiences led us to analyze our data for the evaluation of factors related to spectacles discontinuation among RAE patients whose refractive errors were ≥+2.00 D at the initial visit, but became mild hyperopic (<+2.00 D) or even myopic after refractive shift. Previous studies have reported various results of clinical courses of RAE and associated factors related to the discontinuation of spectacles [1,6,7]. Mohney et al. [1] reported an association of full term birth and low hyperopic error with early discontinuation of spectacles. However, their study included not only fully accommodative esotropia but also partially accommodative esotropia. Lambert et al. [6] noted that the clinical characteristics most clearly associated with successful weaning was the refractive error at the time glasses were prescribed, and the presence of high-grade stereopsis does not seem to be a prerequisite for successfully discontinuing spectacle wear. However, these results came from a very selective group of patients; in particular patients whose refractive errors exceeded +5.00 D were excluded from their study. Although it is not uncommon for RAE patients to have a refractive error of more than +5.00 D, their study did not explain why such patients were not included in the study. In order to minimize limitations of previous studies and meet the aim of our study, first, we analyzed the data of all RAE patients in our clinic no matter what their refractive errors were at the initial visit (the range of initial SE refractive errors of patients included in this study: 2.25 to 8.75 D). Second, partially accommodative esotropia patients who underwent a surgical treatment during follow-up were excluded. In addition, diagnosis and follow-up (of at least 5 years) were made by one strabismologist. We are of the opinion that the clinical data gained by a single clinician will be more valid than that gained by different clinicians.
Hutcheson et al. [15] reported that the baseline and final refractive errors were significantly lower in the children successfully weaned from spectacles. Our results differed from those of this study. In this present study, SE refractive errors did not show any significant association with the discontinuation of spectacles. Differences in SE refractive errors at the initial visit were observed between the two groups, but failed to reach statistical significance. Moreover, the initial and final means of the SE refractive error were higher in the group that showed good ocular alignment without spectacles. A significant difference in stereoacuity measured by the Lang I stereotest was observed between the two groups and was also the factor most associated with spectacles discontinuation in the multivariate logistic analysis. The result of the Stereo Fly Stereotest showed increasing trends towards group A with worsening stereoacuity. These results suggest that stereoacuity might show a greater association with the discontinuation of spectacles, rather than the SE refractive errors. The duration between the onset of esotropia and prescribing spectacles also showed a significant association with the discontinuation of spectacles in the univariate logistic analysis. The duration between the onset of esotropia and prescribing spectacles was shorter in group B. This means that the RAE patients who were prescribed spectacles promptly at the onset of esotropia were more likely to discontinue the use of spectacles. These results demonstrate the importance of early treatment and are consistent with previous studies that emphasized prompt optical correction in the treatment of RAE.
The limitations of our study are as follows. First, the fusional ability was evaluated using the Worth 4 dot test, however, not all patients were tested. Therefore, we could not analyze an association between spectacles discontinuation and fusional ability for the missing observations. This potential relationship would be a topic for further study. Second, our study included patients with RAE who became mildly hyperopic (<+2.00 D) or myopic at the last follow-up. This design of the study allowed for the possibility of selection bias. To overcome this limitation, we reviewed all patients who followed-up during the study period.
In conclusion, our study demonstrated an association of stereoacuity with spectacles discontinuation among RAE patients whose refractive error became mildly hyperopic or myopic after a refractive shift. In addition, the RAE patients who were prescribed spectacles promptly at the onset of esotropia were more likely to discontinue use of spectacles. This result may be helpful in the prediction of spectacles discontinuation in RAE during follow-up.
Notes
This article was previously presented at the annual meeting of the European Strabismological Association, Marseille, France, September 4-7, 2013.
No potential conflict of interest relevant to this article was reported.