Proteus Syndrome: Report of a Case with Developmental Glaucoma
Article information
Abstract
The purpose of this study was to report developmental glaucoma and pseudopapilledema in a patient with Proteus syndrome. We defined the presence of developmental glaucoma, right pseudopapilledema and myopia in a 4.5-year-old patient with Proteus syndrome. Marked right hemihypertrophy, lipoma, macrodactyly, and asymmetry of the limbs were observed on systemic examination. A cavernoma was also detected in magnetic resonance imaging of the brain. The patient underwent bilateral goniotomy surgery due to glaucoma. The surgical outcomes were satisfactory in both eyes. In conclusions developmental glaucoma and pseudopapilledema might be associated with Proteus syndrome.
Proteus syndrome (PS) was first described as a clinical entity by Cohen and Hayden [1] in two patients in 1979. Dietrich et al. [2] titled the disease, which has multiple, diverse, somatic manifestations, as the Greek god Proteus, who could change his form at will. PS is a complex hamartomatous disorder involving the skeletal system, skin, soft tissues, and vascular system. PS is an exceptionally rare and overdiagnosed disorder of mosaic growth dysregulatıon [3,4]. The characteristic signs include partial gigantism of the hands a nd/or f eet, a symmetry of the limbs, plantar hyperplasia, macrodactyly, bony exostoses, soft tissue tumors (hemangioma, lymphangioma, lipoma), varicosities, mental retardation, bony prominences on the skull, scoliosis, kyphosis, angulation knee defects, muscle atrophy, pelvic lipomatosis, verrucous epidermal nevi, and long bone overgrowth [3,4,5,6].
About 200 cases of PS have been reported in the literature, and incidence of ocular malformations is unknown [3]. Fibrous tumor of the superior oblique tendon [7], retinal dysgenesis, retinal pigmentary abnormalities, optic nerve hypoplasia, strabismus and high myopia [3], calcific band keratopathy, cataract, vitreous hemorrhage and resolved serous retinal detachment [8], epibulbar tumor, posterior segment hamartoma, enlarged eye [9,10], and glaucoma [6,10,11] characterize the syndrome. However the ocular manifestations of PS require clarification.
We report herein a patient with developmental glaucoma and pseudopapilledema, presumed to be due to PS.
Case Report
A 4.5-year-old male was referred to our ophthalmology department, due to developmental glaucoma. The prenatal history was unremarkable. On physical examination, marked right hemihypertrophy, a protuberant abdomen containing subcutaneous tumors and lipoma, macrodactyly of the third and fourth digits of the right hand, macrodactyly in nearly all of the toes (Fig. 1), hyperpigmented skin lesions on his back and legs, verrucous epidermal nevi, and asymmetry of the limbs were discovered. Magnetic resonance imaging of the brain showed a temporal lobe cavernoma (Fig. 2). However, there were no neurological symptoms related with the cavernoma.

(A) Right hemihypertrophy, (B) subcutaneous tumors and lipoma, (C) macrodactyly of the third and fourth digits of the right hand, and (D) macrodactyly of nearly all the toes.
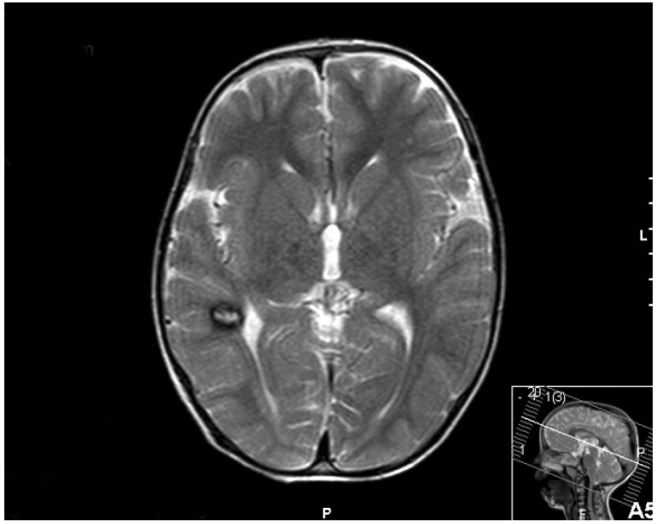
Magnetic resonance imaging of the case, showing temporal lobe cavernoma.
On ophthalmic examination, bilateral developmental glaucoma, unilateral pseudopapilledema, and myopia were detected. The patient had a history of a bilateral goniotomy operation when he was four months old. Visual acuity could not be measured due to mental-motor retardation, but central, steady, maintained fixation (CSM) was positive in both eyes. Slit-lamp examination showed Haab's Striae with a corneal diameter of 11 mm horizontally and 12 mm vertically in the right eye. The left eye was buphthalmic, with a corneal diameter of 12 mm horizontally and 13 mm vertically. Gonioscopy showed grade 4 open angles in both eyes. Intraocular pressures were 12 mmHg in the right eye and 14 mmHg in the left eye with latanoprost 0.005% once a day treatment. Central corneal thickness measurements using ultrasonic pachymetry were 557 µm in the right eye and 509 µm in the left eye. Pseudopapilledema was also detected in the right eye. Cup/disc ratio was 0.5 in the right eye and 0.7 in the left eye (Fig. 3). Axial lengths were 22.8 mm in the right eye, and 25.36 mm in the left eye. Cycloplegic retinoscopy showed -5.50 (-2.50 × 90) diopters in both eyes. Best-corrected visual acuity was 20 / 40 in the right eye and 20 / 50 in the left eye.
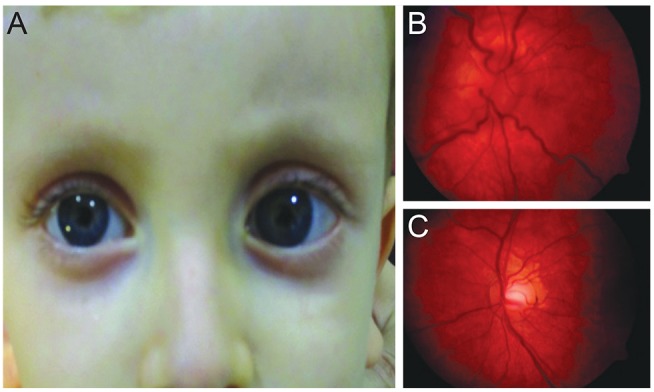
(A) Buphthalmia in the left eye, (B) pseudopapilledema in the right eye, and (C) appearance of left optic disc.
Discussion
PS is thought to occur as the result of a lethal somatic gene mutation that leads to a mosaic state. Most patients with PS are born without significant asymmetry, but some cases were diagnosed using prenatal ultrasonography, and rapidly progressive overgrowth could paused during puberty [7,10,11,12,13,14]. The most common clinical ocular manifestations of the disease have been reported to be strabismus and epibulbar tumors [10,11,12]. In the present case report, we defined a concordance of developmental glaucoma, pseudopapilledema, and myopia in a 4.5-year-old male patient with PS.
Clinical diagnosis of PS is challenging and contentious. In the early stages of the disease, it may be difficult to make differential diagnosis from other overgrowth disorders, such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, Congenital Lipomatous Overgrowth, Vascular Malformations, and Epidermal Nevi (CLOVE) syndrome, and Bannayan syndrome. These disorders may present with similar manifestations as PS; however, they had stringent diagnostic criteria that delineated a distinct cohort of patients who have parallel features of overgrowth [4,13,14]. According to the literature; the prognosis of the PS seems to labile and is correlated to the severity of neurological involvement, skeletal deformities, internal lipomatosis, and neoplastic appearance [8]. Different manifestations suggest that patients with PS should have an ophthalmological examination.
We have defined in the present report that developmental glaucoma and pseudopapileudema in a patient with PS for the first time in the literature. The diagnosis of PS was based on the typical clinical findings including hemihypertrophy, subcutaneous tumors and lipoma, macrodactyly, hyperpigmented skin lesions, verrucous epidermal nevi, and asymmetry of the limbs. Ophthalmologic examination revealed developmental glaucoma which was already treated with goniotomy in both eyes. Although the intraocular pressures were in normal limits with latanoprost 0.005% once a day treatment, left eye enlargement was evident. Although the precise mechanism of the pathogenesis of secondary glaucoma associated with PS is unknown, the most likely explanation is the malformation of the trabecular meshwork and iris (iridotrabeculodysgenesis) or iridocorneal dysgenesis. Hamarthomatous lesions may also be another cause of glaucoma in these individuals.
In conclusion, patients with a diagnosis of PS should be carefully reviewed by an ophthalmologist to rule out ocular manifestations of the disease. Timely diagnosis and treatment of the developmental glaucoma may preserve visual loss in patients with PS.
Notes
No potential conflict of interest relevant to this article was reported.