


Superior oblique palsy (SOP) is one of the most common causes of paralytic strabismus [1]. When the superior oblique muscle (SOM) is paralyzed, the eyeball is deviated inward and upward. Specifically, intorsion is observed considering that the primary actions of the SOM involve intorsion, abduction, and infraduction. In particular, the anterior and posterior parts of the SOM are involved in incyclotorsion and infraduction, respectively [2].
In the case of bilateral SOP, vertical deviation is usually small, and patients with SOP present with V-type esodeviation and bilateral extorted eyes [3]. Cyclotorsion is considered a crucially important feature in the bilateral SOP, and various surgical treatments have been tried to treat bilateral SOP. Among them, in 1964, Harada-Ito surgery was performed to correct isolated cyclotropia [4], and the anterior part of the SOM was pulled laterally without separation and detachment of muscle fibers. Subsequently, several modified methods have been introduced [5].
To increase the success rate of the surgery, an adjustable technique is applied, and the results of the adjustable surgery were favorable [6,7]. However, an adjustable surgery is associated with several complications such as vagal reactions during the adjustment procedure, increased postoperative inflammation, exposed sutures, and slipped adjustable suture knot [8]. Additionally, controversy about the success rate of adjustable suture surgery exists [9,10]. Therefore, we investigated the success rate of nonadjustable modified Harada-Ito surgery.
Materials and Methods
This retrospective study was conducted at a single center. The study was approved by the institutional review board of KimŌĆÖs Eye Hospital (2020-02-006-002) and conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was waived because of minimal risk of personal information. From January 2009 to December 2018, a total of 22 patients underwent Harada-Ito surgery. All patients were diagnosed as acquired SOP and complained of torsional diplopia and did not respond using prism correction. Among them, 21 out of the 22 patients who were followed up for 6 months after surgery were included in this study and one patient were excluded because of short follow-up.
All surgeries were performed by one surgeon. A superior temporal fornix incision was made through the conjunctiva. The superior rectus muscle was isolated using a muscle hook, and the SOM was carefully identified. The tendon of the SOM was divided into half using a muscle hook and Westcott scissors. The tendon split was extended for 10 mm to prevent the interaction between the anterior part and the posterior part of the SOM. The anterior part of the SOM was detached from the sclera and transposed 8 mm posterior to the lateral rectus using a 6-0 Vicryl suture. Finally, conjunctival suture was repaired.
Full ophthalmological examinations were performed. Vertical and horizontal deviations were calculated using the alternate prism cover test. Subjective and objective cyclotorsions were measured. The double Maddox rod test (DMRT) and Lancaster screen test were used to investigate subjective torsion. Objective torsion using fundus photography was measured using the fovea-disc angle method, which was obtained from the angle between one horizontal line passing through the center of the disc and another line between the fovea and the center of the disc (Fig. 1) [11]. The degree of excyclotorsion, which was calculated by fundus photography, was calculated by obtaining the sum of the degree of excyclotorsion from each eye. For example, when the patient has 10┬░ of excyclotorsion in the right eye and 12┬░ of excyclotorsion in the left eye, the summed degree of excyclotorsion is 22┬░.
The success of surgery was defined as follows: success (the patients do not acknowledge diplopia at any direction), partial (the patients feel diplopia at a specific direction, but they do not feel discomfort in routine life), and fail (the patients feel diplopia in primary gaze, hence requiring a thorough investigation).
Comparative studies between the preoperative and postoperative deviations including vertical, horizontal, and torsional deviations were conducted using Mann-Whitney U-test, and subgroup analysis was performed using the analysis of variance test. The chi-square test was used to evaluate the prevalence of objective cyclotorsion after surgery. Statistical analysis was performed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as p < 0.05.
Results
A total of 18 males and 3 females were included in the study, and the mean age of the patients was 56.5 years (range, 40-77 years). Eighteen out of the patients had a history of trauma, and three patients developed diplopia without trauma.
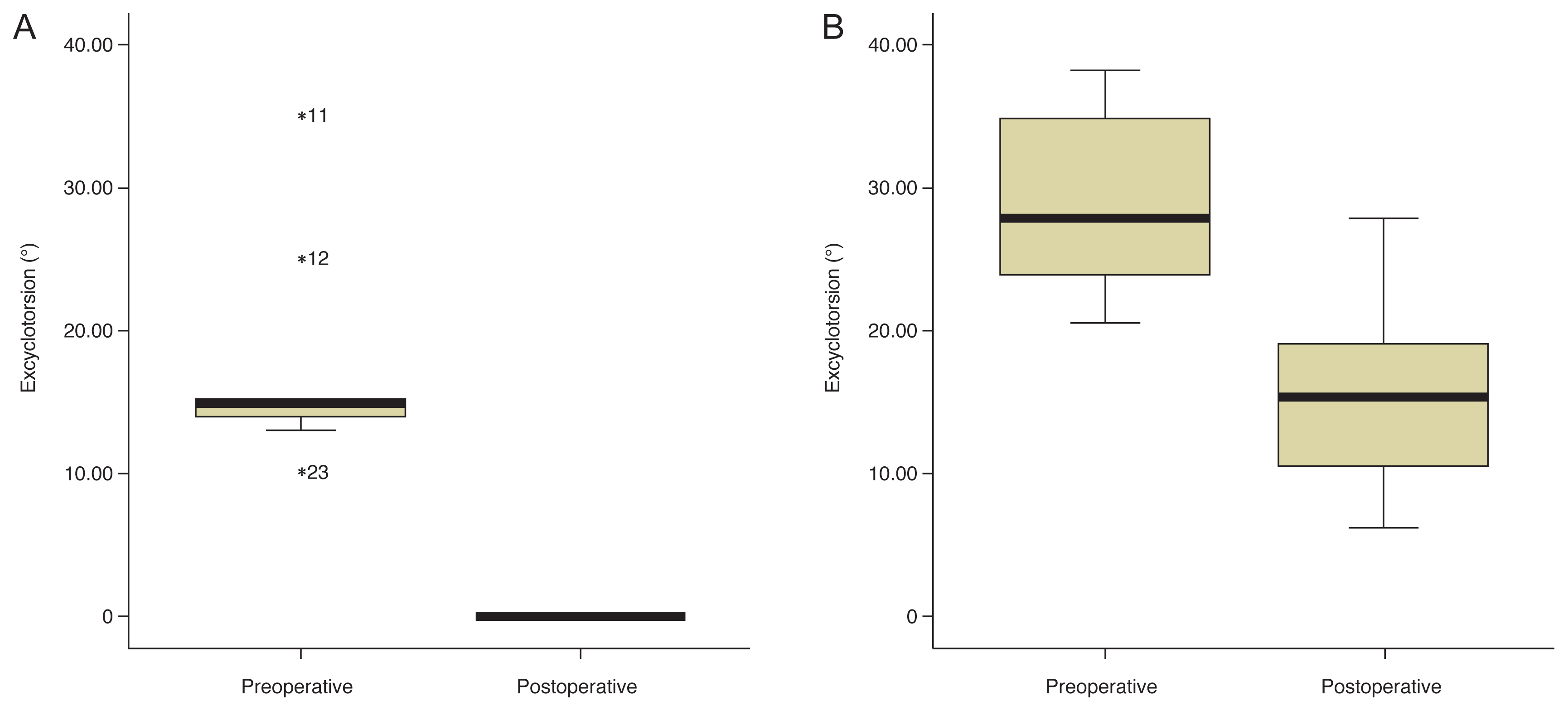
Postoperative examinations were performed at 12.7 months (range, 6-47 months). Based on the alternate prism cover test, the patients had 4.2 ┬▒ 3.0 prism diopters of vertical deviation. Preoperatively, the degrees of excyclotorsion were 14.9┬░ ┬▒ 6.9┬░ and 23.3┬░ ┬▒ 11.0┬░ based on the DMRT and fundus photography, respectively.
After performing modified Harada-Ito surgery, the corrected amounts of cyclotorsion were 14.8┬░ ┬▒ 7.5┬░ and 9.8 ┬▒ 7.9┬░ based on the DMRT and fundus photography, respectively, and were significantly different between the two tests (p = 0.006) (Fig. 2A, 2B). The Lancaster test, which was performed postoperatively, demonstrated that 15 out of the 18 patients had no torsion during the test. However, four out of the 15 patients still complained of diplopia in the secondary gaze.
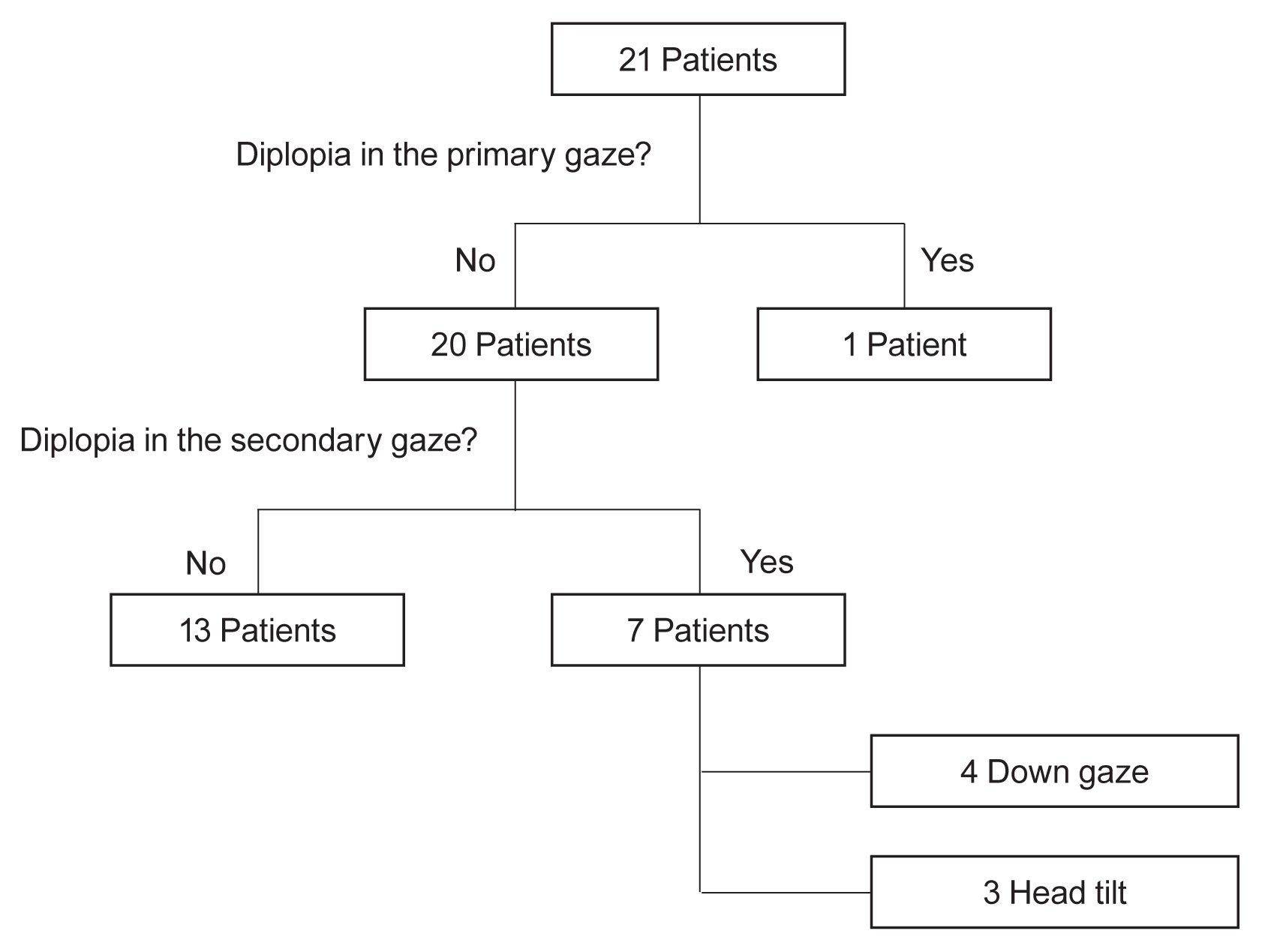
Regarding the success rate of the nonadjustable surgery, diplopia in the primary gaze was resolved in 20 out of the 21 patients (95.2%). However, among these 20 patients, seven complained of diplopia in the secondary gaze (down gaze, four patients; head tilt gaze, three patients). Finally, 13 out of the 21 patients (61.9%) completely recovered after surgery (Fig. 3). Among the four patients with diplopia in downgaze, infra-transposition of the bilateral medial rectus muscle was performed in two patients, resolving diplopia.
The success group had a smaller preoperative subjective excyclotorsion than the partial and fail groups (12.6┬░ ┬▒ 2.5┬░ and 21.0┬░ ┬▒ 8.9┬░, respectively; p = 0.046). However, preoperative vertical deviation and objective excyclotorsion, which was measured by fundus photography, were insignificant between the success group and the partial/fail groups (Table 1).
Discussion
The present study shows that the success rate of nonadjustable modified Harada-Ito surgery is favorable in patients with bilateral SOP.
We performed modified Harada-Ito surgery and this method applied that the anterior half of the tendon was disinserted and sutured at 8 to 10 mm after lateral rectus muscle insertion [5,11,12]. The effect of torsional correction in Harada-Ito surgery varies among authors. Nishimura and Rosenbaum [13] reported that the degree of excyclotorsion correction was 7.3┬░ at 6 months and 5.9┬░ at 1 year. Bradfield et al. [12] presented that the mean degree of torsion correction was 10.3┬░ at the mean 2 years (range, 2-60 months) (bilateral surgery, 12.0┬░; unilateral surgery, 8.4┬░). Ayyildiz et al. [14] reported a higher degree of correction (18┬░-20┬░). The present study noted that the degrees of correction were 14.8┬░ and 9.8┬░ based on the DMRT and fundus photography, respectively. Therefore, the surgeon should have his/her own surgical table to correct cyclotorsion because the difference in the degree of correction is possibly attributed to the surgical technique. A difference in the degree of torsional correction between the DMRT and fundus photography was observed, and the corrected degree of torsion measured by the DMRT was higher than that measured by fundus photography by approximately 5┬░. The difference may be attributed to the torsional vergence amplitude. Torsional vergence varies depending on the gaze. In the primary gaze, the degrees of excyclovergence are 4.15┬░ ┬▒ 1.86┬░ and 2.58┬░ ┬▒ 1.26┬░ with vertical lines and horizontal lines, respectively [15]. Therefore, a safety margin should be considered when correcting cyclotorsion.
The present study revealed that the success rate of the surgery is 95.2%, and the complete resolution rate of diplopia in all gaze directions is 61.9%. The success rate of the surgery is 43% to 73% in all patients [5,12,13]. The definition of success rate of the Harada-Ito surgery varies depending on the studies. When success is defined as no diplopia in the primary gaze and downgaze, the success rate of the present study was 76.2%. Despite the generally high success rate of Harada-Ito surgery, diplopia in a specific gaze, specifically downgaze, is a key problem that needs to be solved [13,16]. The present study showed that four of the 20 patients (20%) complained of diplopia in downgaze. In this case, infra-transposition of the bilateral medial rectus muscles should be performed.
This study has several limitations. First, the follow-up period is relatively insufficient to evaluate the long-term effects of the surgery because the correction degree of excyclotorsion usually regresses over time [13]. Thus, the success rate of the present study might decrease over time. Second, this study did not directly compare the success rate between the adjustable and nonadjustable surgery. However, the favorable success rate of nonadjustable surgery (primary gaze, 95.2%; all gaze directions, 61.9%) is considered significant. The degree of subjective cyclotorsion based on the DMRT is considered as one of the prognostic factors considering that a significant difference between the success group and the partial/fail groups was observed in this study.
In conclusion, nonadjustable modified Harada-Ito surgery has a favorable success rate, and patients undergoing this surgery are considered safe considering that this surgery is performed without additional adjustment procedure.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






