

Coats' disease typically induces idiopathic retinal telangiectasias in all components of the retinal vasculature. In addition, it induces significant lipid deposition due to the non-perfusion of thecapillary blood vessels, aneurysm formation, and subretinal exudation. Adult cases of Coats' disease are often asymptomatic, or the visual acuity at the initial diagnosis is better than in pediatric patients. Leukocoria is absent at the time of diagnosis, and the extent of exudation and retinal detachment tends to be mild.1 Treatment is performed according to, the Shields classification.2 The occlusion of the dilated blood vessels is treated by cryotherapy and laser photocoagulation for stage 1-3A. Surgical retinal reattachment is performed for most cases of stage 3B. Enucleation is indicated for stage 4 patients. In this adult Coats' disease patient, bevacizumab and triamcinolone acetonide were injected into the vitreous in an attempt to resolve the severe macular edema in the submacular area and to facilitate laser photocoagulation on retinal telangiectasias. This procedure has not been reported previously in Korea.
Case Report
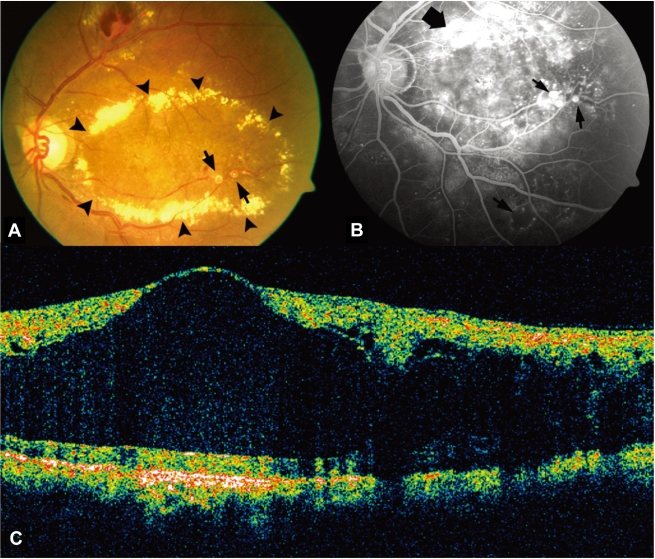
A 47 year old male patient visited our hospital with the chief complaint ofacute progressive deterioration of the visual acuity of his left eye that had begun 2 months earlier. No specific findings were detected in his prior history. Thetotal cholesterol, component ratio of triglycerides, HDL-cholesterol and LDL-cholesterol were within the normal range. At the initial examination, the corrected visual acuity of his right and left eye was 1.0 and 0.02, respectively. The intraocular pressure of the right and left eye, measured using a non-contact tonometer, was 19 mmHg and 16 mmHg, respectively. The slit lamp examination revealed no specific special findings in the anterior segment and no rubeosis. The bilateral fundus examination showed normal findings in his right eye, and thick macular edema in the posterior pole in his left (Fig. 1A). Fluorescein angiography revealed profuse leakage with capillary dropout and a club shape thatdiffused to the blood vessels in the vicinity of the posterior pole (Fig. 1B). OCT showed that the retina thickness had thickened noticeably to 1,187 ┬Ąm as a result of macular edema (Fig. 1C). Focal laser photocoagulation was attempted in the dilated vessel area but it was difficult to perform satisfactorily because of the thick retinal edema. The OCT taken 1 week after his first visit did not show any improvement of the macular edema. Therefore, bevacizumab (AvastinŌäó, 25 mg/ml, 4 ml, Roche, USA) 1.25 mg (0.5 ml) was injected into the vitreal cavity in order to subside the retinal edema and facilitate focal laser photocoagulation on the telangiectatic vessels. Additional focal laser photocoagulation was then performed. However, OCT taken at 3 week visit after the injection showed that the macular thickness had barely changed. On the 6th week after treatment, an intravitreal injection of triamcinolone acetonide (Triamcinolone inj┬«, 40 mg/ml, 5 ml, Dongkwang pharma, Korea) 4 mg (0.1 ml) was performed to resolve the retinal edema for focal laser photocoagulation. One week after the triamcinolone acetonide injection, the visual acuity was 0.02 and showed no improvement. However, there was a noticeable reabsorption of the macular edema. At the 2nd week after the injection, the foveal structures began to recover. After 5 weeks, the retinal thickness had decreased to 244 ┬Ąm (Fig. 2C). The visual acuity improved slightly to 0.04, and additional focal laser photocoagulation could be performed easily and satisfactorily with the absorption of the retinal edema. Repeated focal laser photocoagulation was performed at each visit until 10 weeks after injection, and the retinal edema remained stable. At 6 months, the OCT showed that the macular edema had increased to 680 ┬Ąm (Fig. 2D). However, on color fundus photography, thick circinate hard exudates was much absorbed (Fig. 2A) and, fluorescein angiography revealed a significant decrease in leakage from telangiectactic vessels compared with that performed at the time ofthe initial diagnosis (Fig. 2B). Consequently, repeated injection of triamcinolone acetonide and repeated aggressive laser photocoagulation was planned in order to prevent further progression.
Discussion
Coats' disease develops primarily in young children under the age of 5 years with relatively few reports of adult cases. According to several studies, the progression of Coats' disease is relatively slow in older children or adults, and it shows indolent clinical features.1-5 In adult cases, themean age at the time of diagnosis is approximately 50 years with a male preponderance.1 In the laboratory examinatio hyperlipidemia is frequently encountered as an accompanying condition. However, in this case, the lipid profile was withinthe normal range. Similar to children, the fundus examination shows arteriovenous dilation of the non-perfusion area of the capillary beds as well as subretinal lipid exudate andmacular edema in the vicinity. Moreover, the involved blood vessel area is closer to the macular area than that observed in typical Coats' disease. In addition, there is less lipid exudate, and the retinal hemorrhage can be observed more often in the vicinity of the greatly dilated blood vessels.1,5
The treatment and prognosis of Coats' disease are influenced by the submacular exudates and the extent of retinal detachment. Focal laser photocoagulation or cryotherapy to the dilated blood vessels is the primary treatment for cases without exudative retinal detachment or mild. Drainage of the subretinal fluid, scleral buckling, pars plana vitrectomy can be applied in cases with severe exudative retinal detachment.2,6-8 However, in Coats' patients, the application of focal laser photocoagulation to the leakage area is limited in most cases due to the profuse retinal edema caused by leakage over a wide area. Moreover, the retinal detachment may persist despite surgical treatments in some cases with extravascular fluid pooling in the outer layers over a wide area. Therefore, several treatment strategies have been attempted. Sun et al.9 reported a case of a stage 4 pediatric patient who was unresponsive to scleral buckling and SRF drainage. The patient was treated with an intravitreal injection of anti-VEGF. After injecting the anti-VEGF agent, pegaptanib sodium, the elevated VEGF levels haddecreased markedly and the exudative retinal detachment had improved. However, in our case, there was no improvement of the exudative lesion after the intravitreal bevacizumab injection. Such a result was obtained because the exudative retinal detachment in Sun's case was the increase in vascular permeability caused by the secondarily elevated VEGF due to retinal ischemia. Our case it was Stage 2A according to the Shields classification. In addition, the ischemic area was not wide and there was only a slight increase in level of VEGF. Therefore, it is not surprising that no noticeable improvement was observed after the bevacizumab injection. This means that the increase in vascular permeability in Coats' disease is induced primarily by morphological problems, and an elevated VEGF level could increase the permeability secondarily with the progression of the disease due to advanced retinal ischemia. Consequently, the therapeutic reaction differs according to the change in pathophysiology during disease progression.
Jarin et al.10 reported that an intravitreal injection of triamcinolone acetonide was effective in an adult Coats' patient who was unresponsive to conventional laser photocoagulation due to the presence of severe macular edema. The microcirculation of the retinal blood vessels and edema were stabilized by triamcinolone because it has been shown to be effective against microangiopathy of which Coats' disease is a chronic form.11 However, in previous report, Jonas et al.12 reported two patient with Coats' like features that was unresponsive to intravitreal traimcinolone. The results of our case are similar to Jarin's case. Moreover, in Coats' disease, macular edema develops as a result of leakage due to destruction of the blood-retinal barrier through the loss of vascular endothelial cells and adjacent cells induced by causes yet to be determined. Hence, in addition to VEGF, other cytokines are believed to be involved. Therefore, it is believed that triamcinolone acetonide injected into the the intravitreal cavity suppressed a variety of cytokines and induced some short term improvement in macular edema.
Overall, Coats' disease with severe retinal edema can be treated accurately and satisfactorily by laser photoacoagulation on the targeted leakage area after absorbing the retinal edema through a triamcinolone acetonideinjection. In addition, it is believed that the partial retinal edema that remained after photocoagulation can be improved with an intravitreal injection of triamcinolone acetonide. However, statistical analysis of the effectiveness of the adjunct treatment based on a larger number of cases will be needed.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






