

Molteno introduced the modern glaucoma implant in 1969, and many different types and associated materials have since been developed. Currently, the Ahmed glaucoma valve, the Molteno implant, and the Baerveldt implant are used widely. Most currently available implants have a silicone tube with an outer diameter of approximately 600 ┬Ąm and an inner diameter of approximately 300 ┬Ąm. The inner diameter of the tube is oversized for an approximate 2.0 ┬ĄL/min inflow rate of aqueous humor to the eyeball. Therefore, these current implants are vulnerable to overfiltration of the aqueous humor and resultant hypotony, choroidal effusion or detachment, or hypotony maculopathy [1,2,3,4,5]. To avoid overfiltration, some glaucoma implants were developed with a one-way valve mechanism [6]. Nevertheless, overfiltration remains a frequent and serious problem of implant surgery. Therefore, many surgeons temporarily occlude the drainage tube using an intraluminal stent or tube ligation [7,8,9,10,11]. The large outer diameter of current drainage tubes can induce conjunctival erosion over the tube [12,13]. To reduce the incidence of this complication, various types of tectorial support between the tube and overlying conjunctiva are applied during surgery. Despite this effort, tube exposure is still one of the main complications of implant surgery [5,12,13].
In contrast, a tube with a smaller inner diameter can provide more resistance to fluid flow, and a smaller outer diameter should decrease conjunctival erosion over the tube and the accompanying complications. A shunt with a small diameter, the ExPRESS implant (Alcon Laboratories, Fort Worth, TX, USA), is currently available. It has a short metallic tube with a 50 / 400 ┬Ąm (inner / outer diameter) but is too short to provide resistance to aqueous flow.
In this study, we evaluated fluid flow in microtubes of various sizes (51, 64, and 76 ┬Ąm in inner diameter) and materials (polytetraf luoroethylene [PTFE] and polyether block amide [PEBAX]) under different conditions (air, water, and enucleated pig eyes). In addition, we investigated the effects of an intraluminal stent.
Materials and Methods
Preparation of microtubes
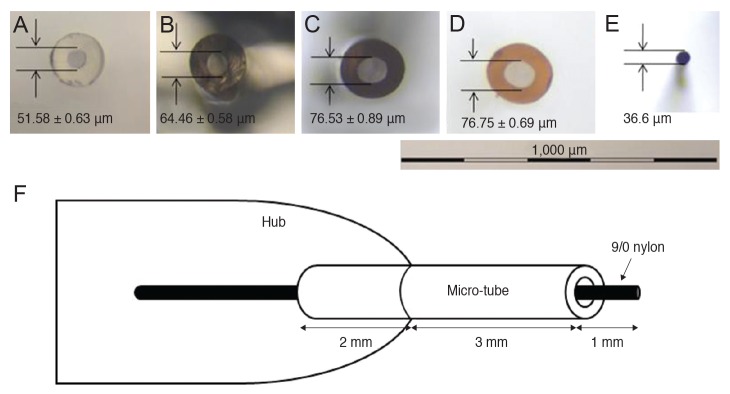
Three extruded PTFE tubes with different inner diameters (51, 64, and 76 ┬Ąm) and one PEBAX tube with an inner diameter of 76 ┬Ąm were tested. We chose 51-, 64-, 76- ┬Ąm extruded PTFE tubes, the three smallest supplied by the manufacturer (Zeus Inc., Orangeburg, SC, USA), and 76-┬Ąm PEBAX tubes. PTFE and PEBAX are significantly different. PTFE has strong lubricant qualities and the lowest coefficient of friction of any known polymer. PEBAX is more flexible than PTFE, is more readily shaped, and can be readily mixed with other materials. All PTFE and PEBAX tubes fulfilled the biocompatibility standards of the United States Pharmacopeia Class VI plastic test. The wall thickness of each tube is 51 ┬Ąm. The tolerances of the inner and outer diameters are ┬▒10 ┬Ąm (provided by Zeus Inc.). Twenty of each of the four tube types were tested (80 tubes in total). Before the experiment, all of the tubes were carefully cut to a length of 5 mm to avoid distortion of the tube. Using a microscope (Optiphot-2; Nikon, Tokyo, Japan) and a measurement program (Prores CapturePro 2.8.8; Jenoptik Optical System, Jupiter, FL, USA), tubes with a less than ┬▒2 ┬Ąm inner diameter tolerance at both distal cut ends were selected for the study. After trimming to a length of 5 mm, the inner diameters of the tubes were 51.58 ┬▒ 0.63, 64.46 ┬▒ 0.58, 76.53 ┬▒ 0.89, and 76.75 ┬▒ 0.69 ┬Ąm (mean ┬▒ standard deviation) for the PTFE tubes of 51, 64, and 76 ┬Ąm diameter, respectively, and the 76-┬Ąm PABAX tube. Fig. 1A-1F shows light micrographs of the cut ends of each tube type and 9/0 nylon.
Device for measuring pressure
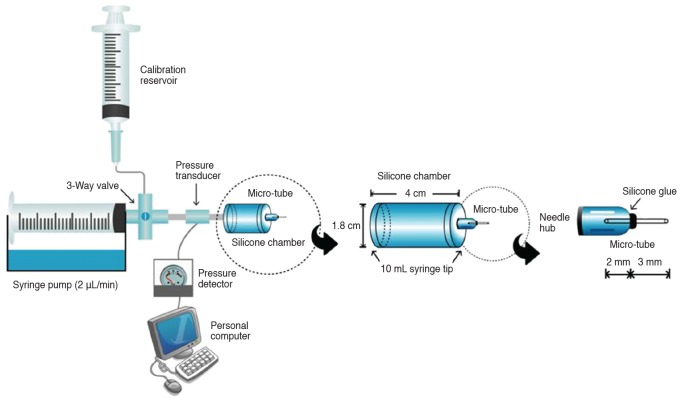
We assembled the equipment to measure pressure due to fluid flow. The definition of pressure in this manuscript is not resistance but maintenance pressure. The device consisted of three components: (1) perfusion pump and syringe, (2) pressure transducer and detector, and (3) silicone chamber and microtube. One perfusion pump and one syringe were connected to two pressure transducers, a detector, a silicone chamber, and a microtube. We ran the two pumps and syringe simultaneously. Therefore, we could simultaneously measure pressures within four microtubes. We adopted a perfusion pump with a stepper motor (Model 11; Harvard Apparatus, Holliston, MA, USA), which was connected to a 1-mL glass syringe (Hamilton, Reno, NV, USA). A three-way valve was connected to the end of the glass syringe, and a calibration reservoir was attached for pressure calibration or air bubble removal. A pressure transducer (PX260; Edwards Lifesciences, Irvine, CA, USA) and detector (8SP; ADInstruments, Colorado Springs, CO, USA) were connected to a personal computer, which monitored the pressure change in units of 0.01 mmHg using Chart v5.1 software (ADInstruments). A 10-mL syringe tip was attached to each side of a cylindrical silicone chamber (length, 40 mm; diameter, 18 mm; silicone thickness, 400 ┬Ąm; volume, 7 mL) with silicone glue. A microtube was attached to the distal end of the silicone chamber using a 30-gauge needle hub after removing the needle shaft. The microtube was inserted 2 mm into the needle hub and fixed in place with silicone glue (Fig. 2). Experiments were conducted after the silicone glue had dried and cured for 2 weeks.
Measurement of pressure
The space within the device was completely filled with distilled water. Air bubbles that formed during the filling process were removed via the calibration reservoir. Calibration measurements were performed using a mercury blood pressure gauge connected to the calibration reservoir [14,15,16]. The syringe pump was set at 2 ┬ĄL/min, and pressure was measured in real-time for 24 hours.
Experimental conditions
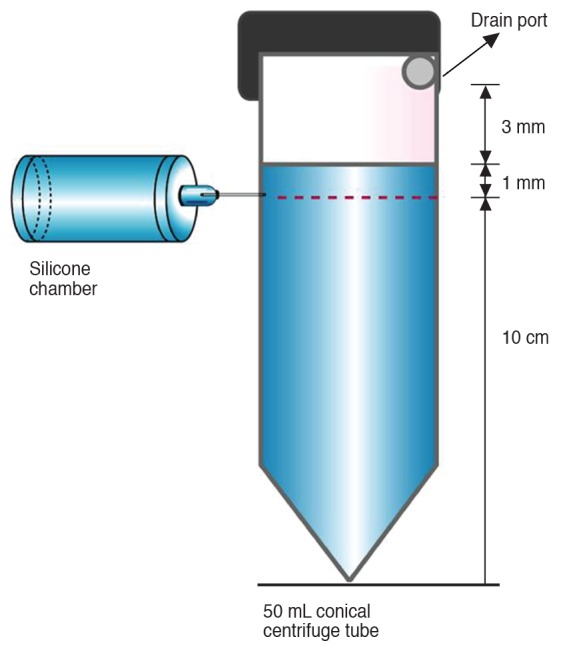
Four tube types of various diameter and material, 20 tubes of each condition, were tested under three different conditions: in air, in water, and in enucleated pig eyes. All experiments were performed at a constant room temperature of 23Ōäā. Measurement of fluid flow was performed first in air (Fig. 2). Then, the distal end of the microtube was inserted 1 mm into a 50-mL conical centrifuge tube filled with distilled water to a level 1 mm above the distal end of the microtube. To avoid an increase in pressure from the increased height of the water surface, an outlet for the water was made 4 mm above the end of the microtube (Fig. 3). Fresh enucleated pig eyes served as an animal model. A limbal-based conjunctiva flap and a Tenon's capsule flap were created, and the distal end of a microtube was positioned on the sclera beneath the two flaps. After confirming that the distal end of the microtube was not occluded by surrounding tissue, the experiment commenced (Fig. 4). The experiments were repeated under the same conditions with a 20-mm length of intraluminal 9/0 nylon (Ethilon; Johnson and Johnson Medical, Cincinnati, OH, USA), and one end of the thread was inserted into the tube 6 mm from the distal end (Fig. 1F).
Statistical analysis
Statistical analysis was conducted using nonparametric statistics with the Kruskal-Wallis test and Mann-Whitney test with SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). In all analyses, p < 0.05 indicated statistical significance. From the continuous 24-hour measurements, the pressures at 10 and 20 hours were collected and compared with regard to the following aspects: (1) the difference in pressure among PTFE tube sizes (51, 64, and 76 ┬Ąm) under each condition; (2) the difference in pressure between PTFE 76 ┬Ąm and PABAX 76 ┬Ąm under each condition; (3) the difference in pressure in tubes of the same size and material at different conditions; and (4) the difference in pressure between tubes with and without the intraluminal 9/0 nylon stent for each tube and condition.
Results
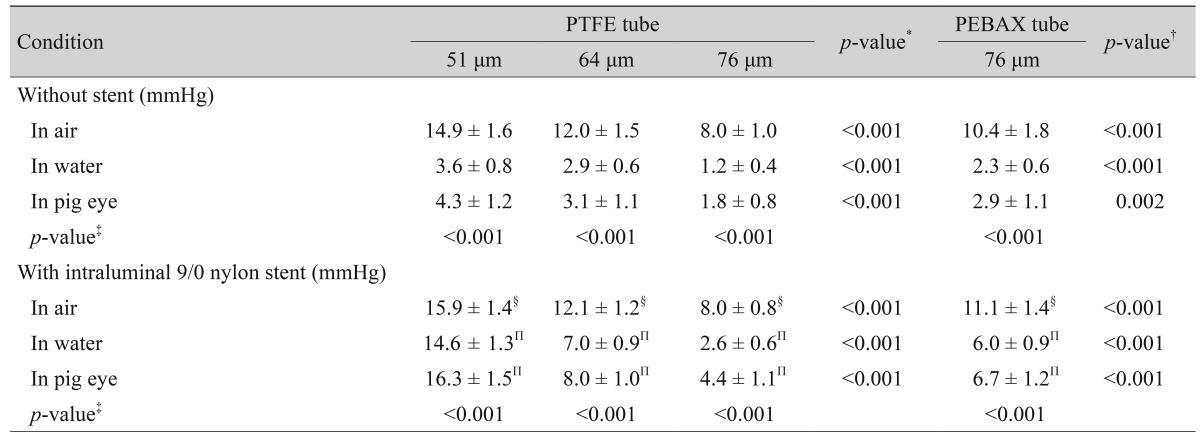
Table 1 shows the mean pressure (mean ┬▒ standard deviation, mmHg) measured for each of the four microtube types 10 hours after beginning the flow under three conditions (in air, water, and enucleated pig eyes). Pressures measured under each condition were much different from the pressure theoretically calculated using Poiseuille's formula for a tube length of 5 mm, inflow rate of 2 ┬ĄL/min, viscosity of 0.932 centipoise (cP), and room temperature of 23Ōäā. The pressures measured under each condition differed significantly among the different PTFE tube sizes. As the diameter increased, the mean pressure decreased, with values of 14.9, 12.0, and 8.0 mmHg in air; 3.6, 2.9, and 1.2 mmHg in water; and 4.3, 3.1, and 1.8 mmHg in enucleated pig eyes, respectively (all p < 0.001). The pressure in PEBAX 76 ┬Ąm was 10.4 mmHg, which was significantly higher than the value of 8.0 mmHg for PTFE 76 ┬Ąm in air (p < 0.001). The pressure was 2.3 and 1.2 mmHg, respectively, in PEBAX and PTFE in water (p < 0.001) and 2.9 and 1.8 mmHg in enucleated pig eyes (p = 0.002). The pressures measured in each tube of the same size and material in air differed significantly from those in water and pig eyes. The pressures were higher in air compared to those in water and pig eyes (all p < 0.001). Pressures measured in the air for the PTFE 51, 64, 76 ┬Ąm, and PABAX 76 ┬Ąm tubes were not significantly different with and without the intraluminal 9/0 nylon stent (p = 0.068, 0.698, 0.779, and 0.289, respectively). However, the pressures measured in water were 14.6, 7.0, 2.6, and 6.0 mmHg for PTFE 51, 64, 76 ┬Ąm, and PABAX 76 ┬Ąm tubes with the intraluminal stent, respectively, which were significantly higher than those measured in the same tubes without the intraluminal stent (3.6, 2.9, 1.2, and 2.3 mmHg, respectively; all p < 0.001). The pressures measured in pig eyes with PTFE tubes of 51, 64, and 76 ┬Ąm diameter and PEBAX tubes of 76 ┬Ąm diameter were comparable to those for intraluminal stents and were significantly higher than those measured without stents (16.3, 8.0, 4.4, 6.7 vs. 3.6, 2.9, 1.2, 2.3 mmHg, respectively; all p < 0.001).
Table 2 shows the mean pressure (mean ┬▒ standard deviation, mmHg) measured for each of the four microtube types 20 hours after initiation of flow under the three tested conditions. The pressures measured under each condition were different from those theoretically calculated using Poiseuille's formula. The pressures measured under each condition differed significantly among PTFE 51, 64, and 76 ┬Ąm. As the diameter increased, the mean pressure decreased (22.1, 16.9, 12.2 mmHg in air; 3.9, 3.0, 1.4 mmHg in water; and 4.6, 3.5, 1.9 mmHg in pig eyes, respectively; all p < 0.001). The pressure in the PEBAX tubes of 76 ┬Ąm diameter in air was 15.8 mmHg, which was significantly higher than the 12.2 mmHg within the PTFE tube of 76 ┬Ąm diameter ( p < 0.001). The values were 2.6 and 1.4 mmHg, respectively, in water and 3.1 and 1.9 mmHg in pig eyes (all p < 0.001). The pressures measured in each tube of the same size and material differed significantly among air, water, and pig eyes; the pressures measured in air were higher than those measured in water and pig eyes (all p < 0.001). The pressures measured in PTFE 76 ┬Ąm and PABAX 76 ┬Ąm tubes with and without intraluminal 9/0 nylon stent were not significantly different when measured in air (p = 0.091, 0.317, respectively), but the remaining pressures with the intraluminal stent were higher compared to those measured without the stent (all p < 0.001).
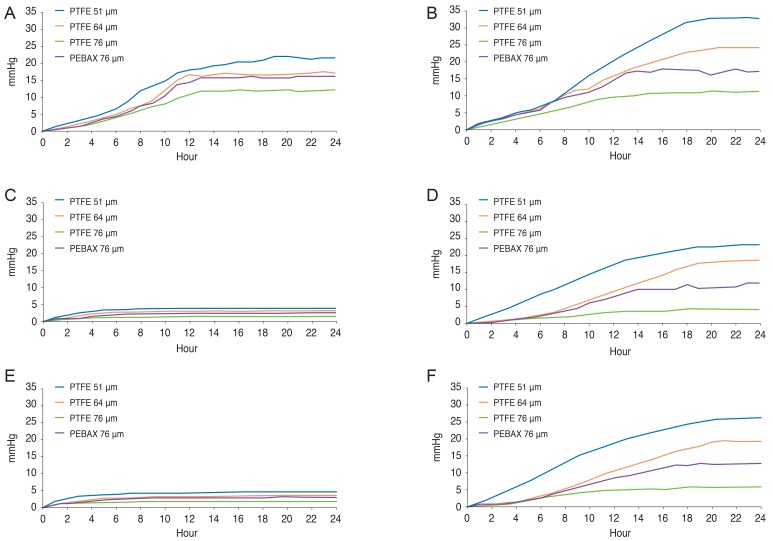
The cumulative pressure profiles are shown in Fig. 5A-5F. Most graphs reached a plateau at 20 hours after initiation of flow. Insertion of the intraluminal stent increased the pressure in the experiments performed in air, water, and pig eyes. When the test was performed within water and pig eyes, the increase in pressure was not remarkable without the intraluminal stent, but the pressure increased markedly upon stent insertion.
Discussion
Most currently available implants in glaucoma implant surgery use a silicone tube with outer / inner diameters of approximately 600 / 300 ┬Ąm. According to Poiseuille's formula, if a tube 15 mm in length with an inner diameter of 300 ┬Ąm is located in an ideal fluid flow system in a given fluid flow of 2 ┬ĄL/min with a viscosity of 0.932 cP (water at 23Ōäā), the pressure difference between the ends of the tube is about 0.02 mmHg [17]. Although the actual in vivo fluid flows are likely to differ from this calculation, this extremely low difference in pressure indicates that the tube itself does not create significant resistance to aqueous flow, indicating the inevitability of overfiltration and hypotony after glaucoma implant surgery. To reduce these complications, a valve mechanism [6], two-stage surgery [18,19], tube ligation, and intraluminal stents have been used in the clinical field [7,8,9,10,11].
Adopting a tube with a smaller inner diameter can provide more resistance to fluid flow due to the size of the tube itself. If it is sufficiently small, the tube can provide a stable intraocular pressure without overfiltration and hypotony after surgery. Recently, a metallic small-diameter aqueous draining tube (ExPRESS tube implant) was introduced. This tube has an inner diameter of 50 ┬Ąm and an outer diameter of 400 ┬Ąm. However, as the length of the tube is only 3 mm, it cannot produce sufficient resistance to the aqueous flow. To our knowledge, there have been no previous reports regarding whether a small tube diameter is the only factor that determines the pressure of microtubes or whether other factors such as the external environment are involved [20].
In the present study, the smallest microtubes with an inner diameter of 51 ┬Ąm and length of 5 mm produced pressures less than 5 mmHg flow in the water and pig eyes, in contrast to the relatively high pressure in air. Experimental conditions cannot exactly duplicate those pressures in vivo. We tested the tubes under three conditions: in air, water, and pig eyes. The latter mimics the conditions in vivo better than the former, in that it can remove the bias in pressure formation caused by the different environment around the end of the tube. These results were similar to those of a previous report by Prata et al. [16], who reported that the maintenance pressure of glaucoma implants was not achieved in fluid (balanced salt solution and plasma) and was higher in air than in fluid. The lower pressures observed in fluids (water and pig eyes) compared to air are likely attributable to the cohesive power and capillarity surface tension of water at the ends of the microtubes [21].
It is difficult to manufacture tubes with an inner diameter smaller than 50 ┬Ąm (outer diameter about 150 ┬Ąm), and it is technically difficult for the surgeon to manage such small tubes. Therefore, increasing the pressure by further reducing the diameter of the tube does not fulfill the basic clinical requirements for tube use. In addition to reducing the tube diameter, additional pressure can be provided by insertion of an intraluminal stent into the microtube, as shown in this study. A 9/0 nylon (diameter about 36.6 ┬Ąm, Fig. 1E) intraluminal stent reduces the cross-sectional inner area of the tube by approximately 1,000 ┬Ąm2. Such a stent can effectively increase the pressure across the tube and can be removed if necessary to increase the aqueous flow after surgery.
Interestingly, the effect of the intraluminal stent was minimaInterestingly, the effect of the intraluminal stent was minimal in the experiment performed in the air. At 20 hours after initiation of flow, the pressure formed by the PTFE 76 ┬Ąm microtube showed an even lower pressure with than without an intraluminal stent, although the intraluminal stent increased the pressure in general. It is postulated that, in the experiment with the large-diameter tube in air, although an intraluminal stent narrowed the lumen, it reduced the frictional force and enhanced flow through the tube. In contrast to the experiments performed in air, those in water showed persistent pressure increases when an intraluminal stent was used. As the diameter of the 9/0 nylon is 36.6 ┬Ąm, a 76-┬Ąm microtube with an intraluminal stent has a cross-sectional area (4,534 - 1,052 = 3,482 ┬Ąm2) similar to that of a 66-┬Ąm microtube (3,419 ┬Ąm2), and a 64-┬Ąm microtube with an intraluminal stent has a cross-sectional area (3,215 - 1,052 = 2,163 ┬Ąm2) comparable with that of a 51-┬Ąm microtube (2,123 ┬Ąm2). However, as shown in Tables 1 and 2, the pressure measured in water and pig eyes for the 64-┬Ąm microtube with an intraluminal stent (7.0 and 8.0 mmHg at 10 hours and 18.0 and 19.0 mmHg at 20 hours, respectively) was greater than that for the 51-┬Ąm microtube without an intraluminal stent (3.6 and 4.3 mmHg at 10 hours and 3.9 and 4.6 mmHg at 20 hours, respectively), despite the larger cross-sectional area of the 64-┬Ąm tube with an intraluminal stent. Therefore, if using an intraluminal stent, factors other than the tube diameter likely influence the pressure.
The pressure also differed according to the tube material in the present study. This may have been due to differences in unevenness of the inner surface or differences in elasticity between PEBAX and PTFE. Hetsroni et al. [22] and Li [23] reported that the uneven internal wall of a tube can increase the pressure by 15% to 37%. In addition, the coefficient of friction may affect the results and changes according to both material and inner diameter of the tube. The coefficient of friction for PTFE is 0.1, whereas that of PEBAX varies between 0.22 and 0.60. In comparison, the reference coefficient range of friction for silicone tubes is 0.25 to 0.75.
A microtube with a very small diameter has some disadvantages for clinical applications, including difficulty of manipulation during surgery and the possibility of tube blockage by tissue debris or inf lammatory materials. Therefore, inserting an intraluminal stent in a relatively large-diameter microtube may be useful in clinical settings, and the diameter can be larger for microtubes made of PEBAX rather than PTFE while maintaining the same pressure.
This study had some limitations. The experimental conditions differed from those in vivo. Distilled water was used for the study, and the experiments were performed at room temperature (23Ōäā). The pressure is affected by viscosity, which changes with temperature. Distilled water is similar to the aqueous humor in terms of viscosity [24], but viscosity may be further altered by the inflammatory response in glaucoma patients during surgery. Because viscosity differs according to temperature (0.932 cP at 23Ōäā and 0.691 cP at 37Ōäā), the pressure at 37Ōäā is 35% lower than that at 23Ōäā [17]. Numerous unexpected factors may affect the pressure in clinical settings. In particular, the pressure at the end of the microtube located within the filtering bleb may be a primary factor affecting fluid flow, and this resistance would be determined in part by the size, height, thickness, and elasticity of the filtering bleb. The pressure of the sub-Tenon's space and the facility of the aqueous outflow through the bleb wall can also affect fluid flow [25]. To explore such in vivo situations, we used freshly enucleated pig eyes. The distal end of each microtube was always placed beneath Tenon's capsule. In addition, elasticity of the eyeball and flow characteristics of the aqueous humor (laminar flow or turbulent flow) can affect the results. Despite these limitations, we compared the relative differences in pressure formed by the different sizes and materials of microtubes under identical conditions, rather than performing precise measurements of pressure. Further studies in a setting similar to the clinical setting are needed to confirm the efficacy and safety of microtubes in preventing overfiltration to avoid hypotony and tube exposure.
In summary, although the pressure can be elevated by microtubes of a smaller diameter in air, reducing the microtube inner diameter to 51 ┬Ąm did not sufficiently increase the pressure measured in water or pig eyes. The external environment around the tube tip and the tube material are important determinants of flow and pressure. Insertion of an intraluminal stent effectively increased the pressure measured in water and pig eyes. PEBAX microtubes afforded higher pressures than did PTFE microtubes.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






