

Is corneal refractive surgery a satisfactory option for doctors who perform sophisticated operations under bright lights or work for a long time under a microscope? Many patients have doubts regarding the safety of this surgical procedure, and worry about postoperative complications. This may be attributable to the fact that most doctors, even those who recommend corneal refractive surgeries for others, traditionally wear glasses.
Functional outcomes and patients' satisfaction after corneal refractive surgeries have been assessed in several previous reports [1-4], and a literature review of studies reporting on the outcomes of laser in situ keratomileusis (LASIK) shows an overall patient satisfaction rate after primary L ASIK surgery of 95.4% [5]. This rate indicates that the vast majority of patients were satisfied with the outcomes of the surgery. Despite the very high success rate, the quality of vision problems such as glare, halo, and subsequent night vision complaints have still been reported in a variety of studies [4,6-8]. In this study, we wished to determine whether physicians who underwent corneal refractive surgery were more dissatisfied with their own outcomes as compared to the satisfaction rate previously reported among general patients, or if they found it more difficult to perform sophisticated operations after the surgery. There have been no reports thus far demonstrating the outcomes and satisfaction rates of physicians who underwent corneal refractive surgery.
The principal objective of this study was to evaluate the satisfaction level of physicians who underwent corneal refractive surgery by comparing the clinical outcomes and subjective satisfaction rates between two groups (physicians and other healthcare workers [HCWs]), and also between two subgroups (medical physicians and surgeons).
Materials and Methods
The study comprised 107 consecutive patients who underwent day-stay LASIK or laser sub-epithelial keratomileusis (LASEK) surgery for the resolution of moderate or low myopia and myopic astigmatism from January 2005 to February 2010 at the Eye Clinical Center of Seoul National University Boramae Hospital. The study protocol was approved by the institutional review board of the Seoul National University Boramae Hospital. All study procedures adhered to the tenets laid out in the Declaration of Helsinki. Patients with keratoconus, other serious preexisting ocular pathology, previous ocular surgery, and history of taking birth control medicine were excluded from this study.
All patients underwent comprehensive preoperative and postoperative ophthalmologic examinations, including measurements of corrected distance visual acuity, uncorrected distance visual acuity (UDVA), slit-lamp biomicroscopy, applanation tonometry, indirect fundus examination, and corneal topography (Orbscan II ver. 3.12; Bausch & Lomb, Rochester, NY, USA). Age, sex, occupations including medical subspecialties, preoperative objective refractions, intraoperative optical zone diameter, postoperative residual spherical equivalent (SE) and residual corneal thickness, and patient satisfaction rate (determined via a questionnaire) were also evaluated.
A 14-question form was adapted from a questionnaire that was previously employed to assess the functional impairment of a broad spectrum of vision-dependent activities carried out in everyday life that can be affected by cataracts (Fig. 1) [9]. The questionnaire was translated into Korean from the original English. The translation process and its validation were carried out as follows. The Korean version was translated into English, and then translated back into English by two different translators. The original and backtranslated versions were compared, and minor inconsistencies were corrected. The translation was carried out after the full validation of the questionnaire had been completed. Patients were required to respond to all questions, and the scale scores increased with satisfaction, ranging from 0 to 4. A score of 4 was assigned when patients reported "no difficulty" with the activity; a score of 3, 2, or 1, when patients reported "a little", "a moderate amount", or "a great deal" of difficulty with the activity, respectively; and a score of 0 when the patients were "unable to do" the activity as the result of their altered vision. No neutral responses were accepted. All questionnaires were mailed or emailed to the patients at 3 months postoperatively, and the data from these questionnaires was compiled by a research assistant (JWK) who was not involved in the patients' clinical care. Patients were also informed prior to completing the questionnaires that the individual results of the study would be compiled by the research assistant, with individual responses remaining anonymous to the clinicians who provided the health care. The patients were, encouraged to answer as truthfully as possible.
LASIK or LASEK procedures were carried out by a single surgeon (YKH). Patients were instructed to discontinue the use of soft contact lenses for at least 1 week and rigid gas permeable contact lenses for at least 3 weeks prior to surgery. LASIK was performed only if the expected residual corneal thickness was more than 250 mm and LASEK was performed only if the expected residual corneal thickness was more than 350 mm. The proper refractive surgery procedures were selected based on the refractive status, corneal thickness, pupil size, and individual patient preference.
All procedures were conducted in accordance with standard protocols and were not customized. LASIK surgery was carried out as described below. After three instillations of Alcaine (propacaine hydrochloride 0.5%; Alcon Lab., Fort Worth, TX, USA), a superior hinge corneal flap of approximately 130 or 160 ┬Ąm was created using a Zyoptix XP microkeratome (Bausch & Lomb). Laser ablation was conducted using a Technolas Z100 Excimer laser machine (Bausch & Lomb). After ablation, the flap was replaced and irrigated with a balanced salt solution. Meanwhile, LASEK surgery was carried out as described below. After three instillations of Alcaine, an alcohol solution cone with a diameter of 8.5 mm (J2905A; Janach, UK) was placed on the cornea. A 20% alcohol solution diluted with distilled water was applied on the cone. After waiting for 30 seconds, the addition of balanced salt solution, and thorough washing were conducted sequentially. Subsequently, using an epithelial micro-hoe (J2915A; Janach, UK), the corneal epithelium was smoothly resected. At a later time, the corneal epithelial flap was gathered in a 12 o'clock direction using a spatula. After irradiation with an excimer laser (Technolas 217Z100; Technolas GmbH Ophthalmologische Systeme, Feldkirchen, Germany), the corneal epithelial flap and the corneal stroma were washed sufficiently with a balanced salt solution and placed carefully in the original site with a spatula. Emmetropia was the end target in every eye.
Cravit (Levofloxacin 0.3%; Santen Pharm., Osaka, Japan) and Flarex (Fluorometholone 0.1%, Alcon Lab.) eye drops were administered 4 times a day for 1 month to LASIK patients. Meanwhile, Cravit drops 4 times a day for 1 month, Ocufen (Flubiprofen sodium 0.03%, Bausch & Lomb) drops 4 times a day for 1 week followed by Flarex drops 4 times a day for 3 weeks were recommended for LASEK patients. Flarex was tapered off twice a day for the next 1 month, and then once a day for an additional month. However, the Flarex drops were tapered off more slowly if patients had evidence of severe subepithelial haze and refractive regression. On the other hand, the drops were stopped earlier if the patients had evidence of no subepithelial haze or refractive overcorrection. All patients were instructed to use preserve-free artificial tear drops and ointment for more than 3 months. Patients were seen postoperatively at 1 day, 1 week, and 1, 2, and 3 months.
Patients were divided into two groups according to their occupations; physicians and other HCWs group who work under a similar working environment. The physicians group included 51 patients (100 eyes) and the HCWs group included 56 patients (112 eyes). The physicians group was also subdivided into two different groups, surgeons or doctors using microscopes (group A) and medical physicians (group B), in order to determine whether there was any difference in satisfaction levels among the physicians according to the subspecialty in which they were currently engaged. Data were collected and analyzed to compare the clinical outcomes and subjective satisfaction rates between groups.
All statistical analyses were performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA), with p-values of Ōēż0.05 considered statistically significant. Chi-square analysis was used to compare the results of various groups, and Student's t-tests were used to compare the means.
Results
Patient baseline characteristics are listed in Table 1. A total of 107 patients were included with a mean age of 28.36 ┬▒ 3.79 years (range, 23 to 41 years). There were 17 males and 90 females. The mean ┬▒ SD preoperative refractive error (SE) was -4.75 ┬▒ 1.69 diopters (D; range, -1.38 to -8.63 D). Of the 107 subjects included in this study, 105 subjects underwent bilateral LASIK or LASEK procedures; 2 (1.87%) were treated only in one eye. Both of the patients in whom only one eye was treated belonged to the physicians group. 35.3% of patients in the physicians group and 5.4% in the HCWs group underwent LASIK. No significant differences in preoperative parameters, including sex, age, and spherical equivalent, were noted between the physicians and HCWs groups. However, we detected a statistically significant difference between the two groups in terms of the ratios of the type of refractive surgery.
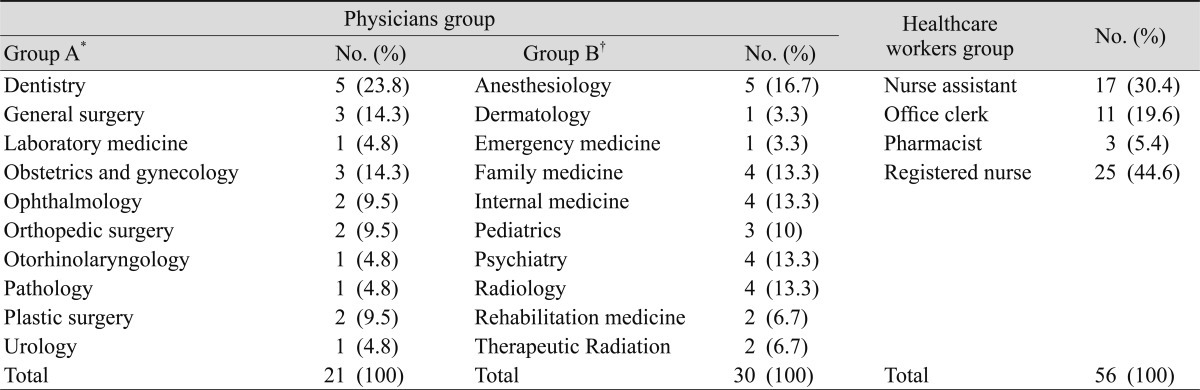
The physicians group had various medical subspecialties. Group A (surgeons or doctors using microscopes) included 21 patients, and dentistry was the most common surgical subspecialty accounting for 23.8% of that group. Group B (medical physicians) included 30 patients, and anesthesiology was the most common medical subspecialty accounting for 16.7%. Of the 56 patients in the HCWs group, 25 were registered nurses and 17 were nurse's assistants, which represented the most common and the second most common occupation in this group, respectively (Table 2).
At an average of 1 month postoperatively, no significant differences were noted in UDVA, residual spherical equivalent, optical ablation zone diameter, and residual corneal thickness between the physicians group and the HCWs group. The difference in residual corneal thickness between the two groups was not statistically significant, but was marginally significant ( p = 0.055). The ratio of LASIK-treated patients to LASEK-treated patients was higher in the physicians group than in the HCWs group. Therefore, the difference in residual corneal thickness is assumed to be associated with this (Table 3).
A sample of the questionnaire and rating scales are provided in Fig. 1. This 14-item questionnaire assesses the extent to which the functional activities of daily living are impaired by visual deterioration. A lower index score corresponded with a lower level of satisfaction, whereas a higher index score corresponded to a higher level of satisfaction. One hundred percent of patients included in this study responded to the questionnaire.
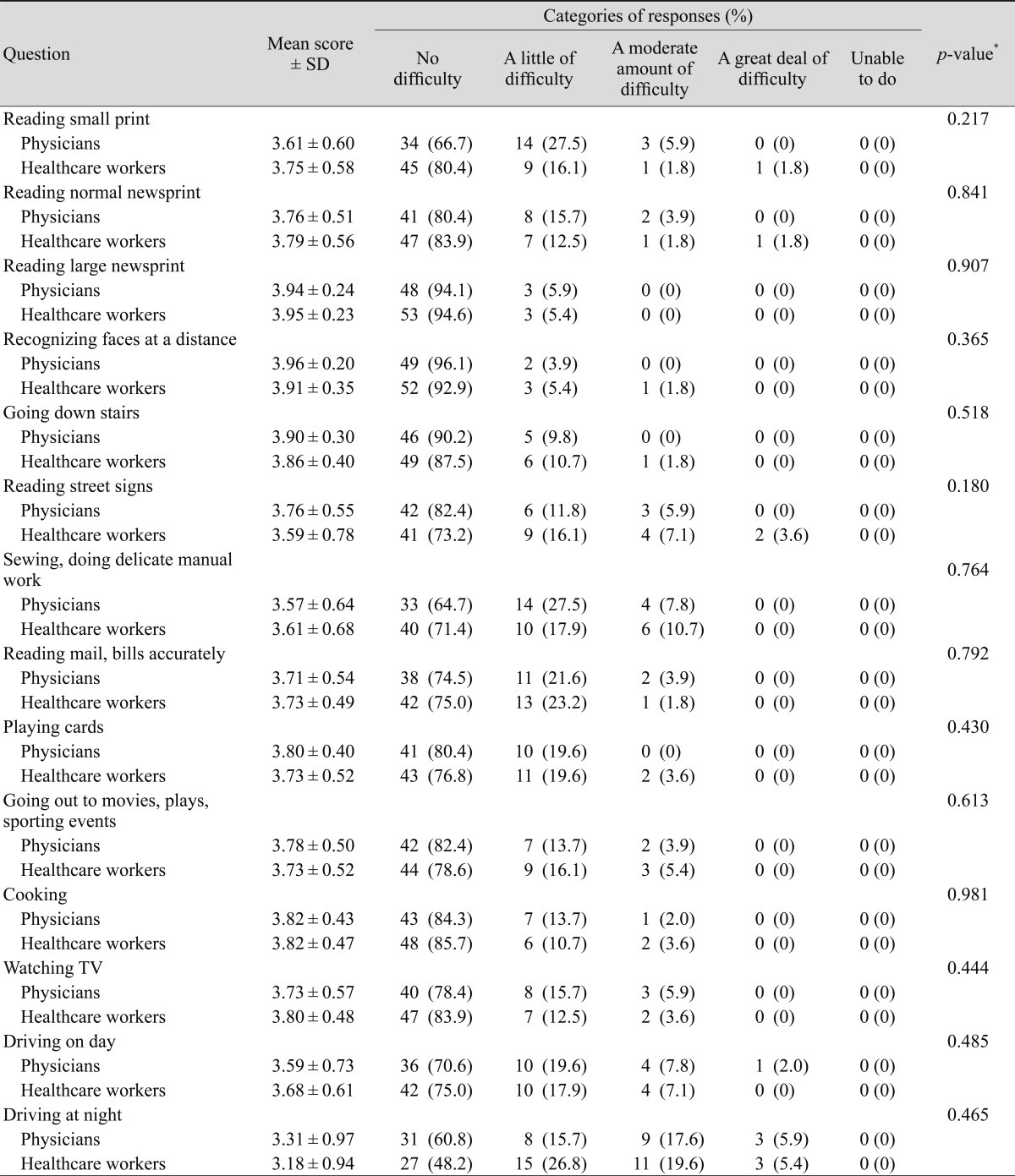
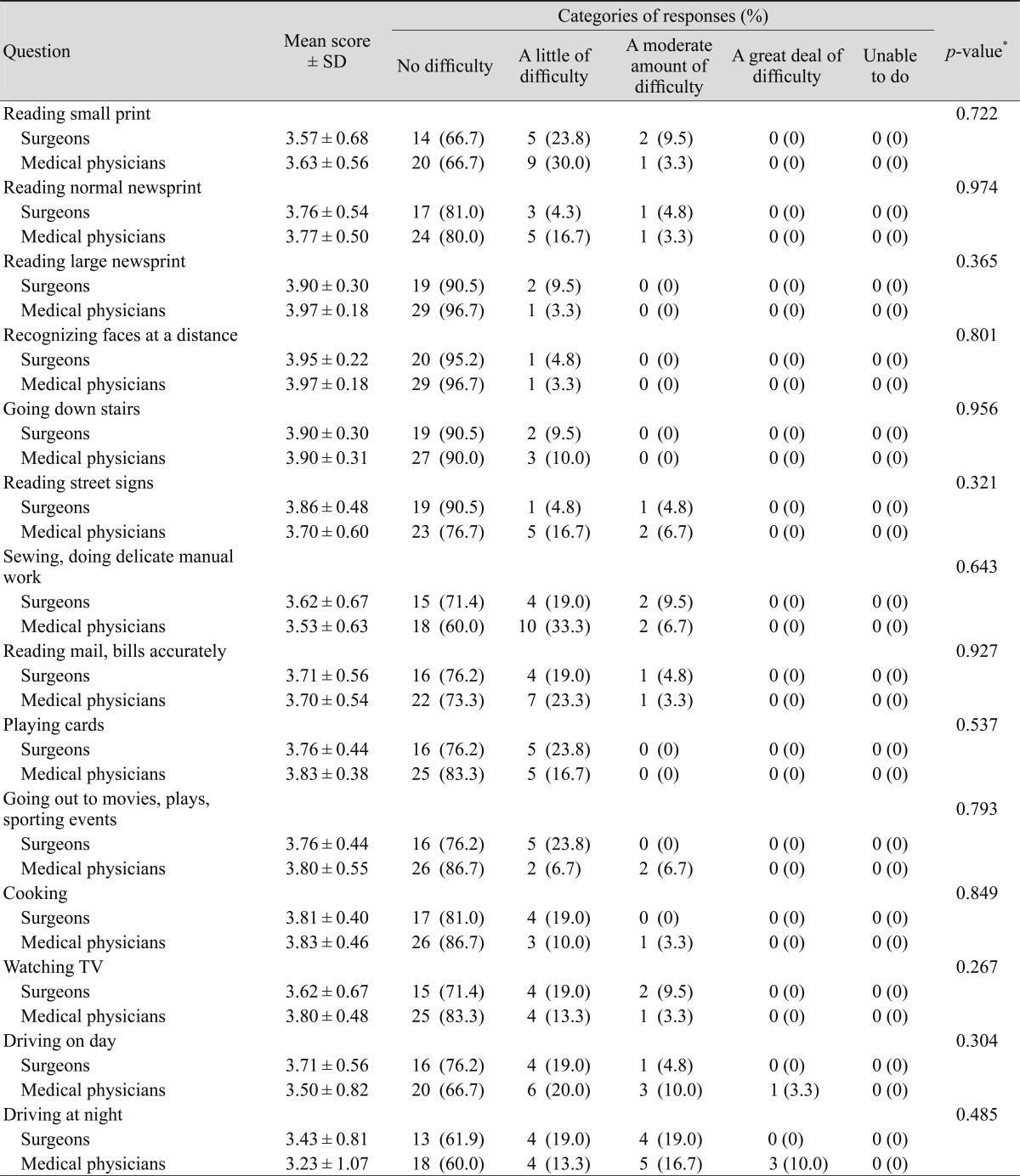
Tables 4 and 5 show the patient responses to the questionnaire. Generally, patient satisfaction rates were high, with a score range of over 3.5 for most of the questions. Overall, the two items with the highest scores were (in order): reading large newsprint and recognizing faces at a distance; the mean scores were 3.94 ┬▒ 0.23 and 3.93 ┬▒ 0.28, respectively. On the other hand, the two items with the lowest score were (in order): driving at night and sewing, and doing delicate manual work; the mean scores were 3.24 ┬▒ 0.95 and 3.59 ┬▒ 0.66, respectively. We noted no significant differences in the mean scores between the physicians group and the HCWs group with regard to the 14 questions used to assess satisfaction with the treatment (Table 4). Table 5 shows the comparison of patient responses between the surgeons group and the medical physicians group. No significant differences were noted in the mean scores with regard to all fourteen questions including the items of sewing, or performing delicate manual work.
Discussion
Overall, many studies have reported excellent medical and functional outcomes in terms of predictability, efficacy, and safety after corneal refractive surgery [1]. Consequently, this has led to high patient expectations and high patient satisfaction rates. However, despite the excellent outcome results and high rates of patient satisfaction, surgical complications remain a problem. LASIK complications include anatomic complications such as corneal flap irregularities, epithelial ingrowth, and keratectasia, refractive complications such as incorrect refractive outcome, irregular astigmatism, decentration, and visual aberrations, functional complications such as dry eyes and increased glare and halos, and infection and inflammatory complications such as diffuse lamellar keratitis [10].
Besides the complications discussed previously, another reason which makes many patients hesitate about corneal refractive surgery is that many doctors, including ophthalmologists, continue to wear glasses themselves, even as they confidently recommend the surgery to patients. However, some bias may underlie this phenomenon. Most of the doctors who patients encounter are largely in the presbyopic (over 40 years) age group, and thus naturally are relatively less likely to undergo refractive surgery. In this study, no patient in the physicians group and one patient (1.8%) in the HCWs group were of presbyopic age, and 4 patients (7.8%) in the physicians group and 6 patients (10.7%) in the HCWs group were of pre-presbyopic age (over 35 years of age).
Young physicians, who stick with glasses and do not generally wish to undergo corneal refractive surgery, tend to think that near vision has some advantage for individual doctors' work, such as reading small print, doing microscopic examinations, or performing microsurgery. In our study, patient satisfaction rates were quite high in regard to distant vision-dependent activities, such as reading large newsprint and recognizing faces at a distance, but were relatively low in near vision-dependent activities, such as sewing, doing delicate manual work, and reading small print. However, no significant differences were noted between the physicians group and the HCWs group in the satisfaction rate, even in terms of near vision-dependent activities. Finally, surgeons who carry out delicate operations might think that once a relatively common complication, such as increased glare and halos, has occurred that it would represent a fatal blow to the surgeons' job skill. This would be applied not only to physicians, but also to other jobs that require near, delicate work skills. In our study, the item with the lowest score was driving at night and night vision symptoms such as glare and halos. These symptoms might be a cause for concern to physicians, especially surgeons. However, there were also no significant differences in the satisfaction scores between the physicians group and the HCWs group in regard to this item, and also between the surgeons and medical physicians groups. Based on these results, it appears reasonable to postulate that corneal refractive surgery can be a recommended option, even for physicians. They appeared to do quite well with intensive near vision-dependent activities and delicate operations, contrary to the general assumptions in this regard.
Our study used a self-administered questionnaire that was sent to patients by an independent research assistant without verbal encouragement. We believe that self-administered tests, as opposed to physician-administered tests, allow for a more objective view of patient satisfaction. We also assigned the control patient group as HCWs who work under a similar temperature, humidity, and other working environmental factors. The registered nurse and nurse assistant, who comprise a large portion of the HCWs group, are occupations that require more distant vision-dependent activities for looking after patients as compared to the physicians group. We believe that these comparisons, with similar working environments but different types of vision required for the performance of job tasks, enable us to analyze the clinical outcomes and subjective satisfaction levels after refractive surgery in a much more reasonable fashion.
Our study was limited in several ways. First, the ratio of LASIK-treated patients to LASEK-treated patients differed significantly between the physicians group and the HCWs group. This is the consequence of different individual patient preference between the two groups. Most of the physicians enrolled in this study were residents or doctors-in-training with very little free time. Thus, they tended to prefer LASIK surgery, which has the advantages of less pain and faster visual recovery. In this study, we did not compare postoperative pain and discomfort, visual recovery time, or dry eye symptoms, all of which depend on the surgical methods used. Therefore, it appears safe to say that this study would be a reasonable method to compare clinical outcomes and subjective satisfaction rates between the two groups, even when the ratio of LASIK: LASEK-treated patients differed significantly. Second, the questionnaire we employed may have been composed of too few items, as it was basically used for cataract patients. Recently, more questionnaires have been developed for refractive surgery patients in order to more fully explore the components and associations of satisfaction [1,2,4,11,12]. In future studies, it should prove interesting to ask new questions evaluating the quality of life, or to address the subjects' level of willingness to recommend corneal refractive surgery to friends.
There were also two ophthalmologists in the physicians group. One of them reported no difficulty (a score of 4) with any of the activities listed in the questionnaire, and the other reported no difficulty with any of the activities except driving at night (with a score of 3). These days, the number of physicians, including ophthalmologists, who have undergone corneal refractive surgery, is increasing. There are no exact statistics regarding the number of physicians that have undergone refractive surgery thus far, but one of the main reasons for the increase in this number might be that physicians themselves believe that this surgery can help perform their job tasks and improve their quality of life.
In conclusion, this is, to the best of our knowledge, the first study ever to evaluate the clinical outcomes and satisfaction rates of physicians who underwent corneal refractive surgery. Even though there was a publication in the literature looking at groups with visually demanding jobs such as military personnel [13], there has been no report regarding physicians. There were no statistically significant differences in the objective clinical outcomes and subjective satisfaction scores after surgery between the physicians group and the HCWs group, and also between the surgeons subgroup and the medical physicians subgroup. Thus, it appears that corneal refractive surgery can be a recommended option even for physicians who must perform intensive near vision-dependent activities, as well as delicate operations. Further study will be required to determine whether the results in this study can be replicated in patients with many more questionnaires and long-term follow-ups.



 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






