

Choroidal detachment (CD) associated with rhegmatogenous retinal detachment (RRD) is a rare condition.1-4 In the majority of cases, CD occurs after the development of RRD. Previously reported risk factors for CD in RRD patients include high myopia, aphakia, pseudophakia, and advanced age.2,5 To the best of our knowledge, however, no studies have yet been conducted regarding the association of macular hole with the development of CD in RRD patients. This study was designed to determine whether the presence of macular hole constitutes a predisposing factor for the development of CD in RRD patients.
Materials and Methods
Patients undergoing operations at the Samsung Medical Center from January 2001 to June 2006 for the treatment of RRD were subjected to searching by the electronic medical recording system of the hospital. Systemic chart reviews were conducted for the searched cases, and the cases which underwent initial operation for RRD at this hospital were included in this study. Thus, the cases undergoing reoperation for recurrent RRD as an initial operation at this hospital were excluded from this study. Cases involving traction-rhegmatogenous retinal detachment, as seen in diabetes, and congenital ocular syndromes with the potential to induce vitreoretinal abnormalities were excluded from this study. The RRD cases which developed after intraocular surgery or penetrating ocular trauma were also excluded. However, cases of RRD detected after cataract extraction were not excluded from the present study. When both eyes were subjected to operation in this hospital for the treatment of RRD during this period, the eye in which RRD was detected earlier than the fellow eye was included.
Although causative retinal breaks were preoperatively identified in the majority of cases of RRD, the eye in which the break was intraoperatively detected was also included in this study. The diagnoses of CD in the eyes with RRD were dependent on both ophthalmoscopy and ultrasonography of the orbit. In one case, CD was detected intraoperatively, and this case was also included in the CD group. The presence of macular hole was diagnosed via slit lamp biomicroscopic examinations utilizing a 90 diopter lens, and was confirmed via optical coherence tomography, with the exception of the cases in which the optical scanning of the macular area proved impossible as the result of media opacity or severe retinal folding. In those cases, the presence of macular hole was intraoperatively confirmed.
Age, sex, preoperative and postoperative best-corrected visual acuity (BCVA), refractive error, intraocular pressure (IOP), systemic disease (i.e., diabetes mellitus and hypertension), lens status, and the presence of macular hole were evaluated with regard to the incidence of CD. Snellen visual acuities were converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. The statistical analysis was conducted using SPSS 11.0 (SPSS Inc., Chicago, Illinois) for Windows software. All tests were two-tailed, and p values of less than 0.05 were considered to be significant. Mann-Whitney's U test and Fisher's exact test were utilized for the analysis of parameters. Multiple logistic regression analysis was employed in order to assess the association between the development of CD and the baseline characteristics. The odds ratio and 95% confidence interval were reported.
Results
This study included 480 eyes with RRD from 480 subjects (193 male and 287 female) with a mean age of 46.1 years (range, 5 to 88 years). Seventy-eight patients (16.3%) evidenced systemic hypertension and 40 patients (8.3%) had diabetes mellitus. Three hundred eighty seven eyes (80.6%) were phakic, 81 patients (16.9%) were pseudophakic, and 12 patients (2.5%) were aphakic. The mean (┬▒ standard deviation) IOP was 12.1┬▒4.7 mmHg in the RRD eyes prior to any treatment.
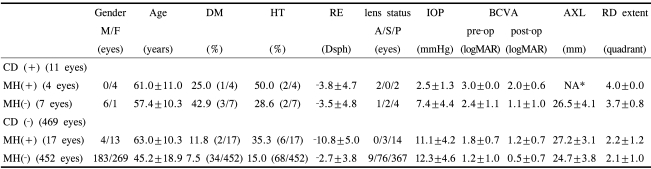
Out of 480 eyes with RRD, 11 eyes involved CD. In 4 of these 11 eyes, the retinal detachment was combined with macular hole. These four cases were all female, and the age was 61.0┬▒11.0 years. In 7 eyes, the development of RRD and CD was unrelated to macular hole. These developed in 6 men and 1 woman with a mean age of 45.2┬▒18.9 years. There were 21 eyes of RRD combined with macular hole. The incidence (4/21 eyes; 19.0%) of CD in the RRD patients with macular hole was significantly higher than that (7/459 eyes; 1.5%) observed in the cases of CD in the RRD patients without macular hole (p=0.010). Table 1 shows the distribution of the studied eyes with regard to the presence of CD and macular hole.
Age, gender, lens status, refractive errors, systemic disease including diabetes mellitus and systemic hypertension, visual outcomes, and IOP were also correlated with the incidence of CD. The eyes complicated by CD evidenced poorer pre- and postoperative logMAR visual acuity (2.5┬▒0.9 and 1.5┬▒1.0) than was observed in the eyes without CD (1.2┬▒1.0 and 0.5┬▒0.7) (p=0.000 and p=0.019, respectively). The preoperative mean IOP (2.5┬▒1.3 mmHg) in the RRD patients evidencing a combination of CD and macular hole was significantly lower than that (7.4┬▒4.4 mmHg) measured in those with CD, but without macular hole (p=0.035). Odds ratio (OR) with a 95% confidence interval (CI) was calculated for each putative predictive factor for the development of CD: macular hole, gender, diabetes mellitus, hypertension, IOP less than 10 mmHg, lens status, and refractive error. Macular hole (p=0.010, OR 22.6, 95% CI 2.1 .240-4), diabetes mellitus (p=0.024, OR 11.8, 95% CI 1.4-100.7) and IOP less than 10 mmHg (p=0.020, OR 8.7, 95% CI 1.4-53.7) were significant factors for the development of CD (Table 2).
There were 17 eyes with RRD coupled with macular hole, but without CD. The mean age of these patients was 63.0┬▒10.3 years. The preoperative IOP (2.5┬▒1.3 mmHg) in the eyes with macular hole and CD was also significantly lower than that (11.1┬▒4.2 mmHg) observed in the eyes with MH, but without CD (p=0.001).
The same parameters were analyzed in accordance with the incidence of RRD caused by macular hole. The significant predisposing factors for macular hole were high myopia (p=0.000), old age (p=0.001), and CD (p=0.002).
For the 11 eyes with combined CD and RRD with or without macular hole, pars plana vitrectomy was conducted in 10 eyes and scleral buckling and subretinal fluid drainage was performed in one eye. Retinal reattachment was achieved after the first operation, in all but 2 eyes. For the 2 eyes with primary failure, macular buckling was conducted in one eye to seal the reopened macular hole, and silicone oil was injected into one eye without macular hole. Finally, retinal reattachment was achieved in all 11 eyes evidencing combined RRD and CD.
In 4 eyes evidencing combined CD and macular hole, preoperative BCVA was equal to or less than the counting finger, and the postoperative BCVA was the same or less than 20/800. In cases of combined CD and RRD without macular hole, the preoperative BCVA of 5 eyes among 7 eyes was equal to or less than hand movement, but the postoperative BCVA of 6 eyes among 7 eyes was improved to better than 5/200.
Discussion
The occurrence of CD in RRD is rare and has been reported in 2% to 4.5% of cases.1,2 In our study, 11 (2.3%) of 480 eyes evidenced CD associated with RRD and the incidence of this is similar to that observed in the previous reports. Although the pathogenic mechanisms of combined CD and RRD has yet to be clearly delineated, most authors agree that the hypotony induced by ciliary edema and the detachment associated with RRD may induce CD.2,6,7 The prognosis for combined CD and RRD is worse than that of uncomplicated RRD.1,2,5,8 This unfavorable prognosis has been attributed to factors including poor visualization, difficult identification of causative break, difficult application of retinopexy, and the development of proliferative vitreoretinopathy.1,2,5,9 Serum components including fibronectin and platelet-derived growth factor were elevated in the vitreous as the result of the extensive breakdown of the blood retinal barrier in eyes with preoperative CD.2,10-13 These factors promote proliferative vitreoretinopathy. Conventional scleral buckling for the treatment of RRD combined with CD was associated with a high incidence of proliferative vitreoretinopathy and an unfavorable reattachment rate, varying from 35% to 62%.1,2,5,14 Thus, as it has been shown to achieve a superior success rate, vitrectomy has usually been adopted as an initial approach for this condition.6,7,15-17 All eyes, with the exception of 1 eye were also treated initially with vitrectomy in this study.
The previous studies showed that the predisposing factors for the development of CD in eyes with RRD included high myopia, aphakia, pseudophakia, and old age.2,5 However, no reports have yet been filed implicating macular hole as a risk factor for CD associated with RRD. As was confirmed herein, the incidence of CD was significantly higher in RRD patients with macular hole than in those without macular hole. This interesting finding shows that macular hole may constitute a risk factor for the development of CD in patients with RRD. Due to the small number of cases, we were unable to determine the manner in which macular hole may increase the risk of CD. We suspect that the high incidence of CD observed in RRD patients with macular hole might be associated with the location of the retinal break and the posterior vitreous detachment. In the typical progression of posterior vitreous detachment, the cortical vitreous separates initially from the retina at the posterior pole, and may then progress in an anterior direction until it reaches the posterior margin of the vitreous base. In cases involving peripheral retinal breaks, the break could be clogged by the overlying vitreous gel as the retina elevates from the underlying retinal pigment epithelium. It may, in turn, limit the progression of retinal detachment, or even, albeit rarely, result in spontaneous retinal reattachment.18 In cases of RRD with macular hole and posterior vitreous detachment, the overlying vitreous gel above the macular hole is absent and the macular hole remains constantly open. Thus, the liquefied vitreous passes through the macular hole uninhibited and is absorbed by the retinal pigment epithelial pump. IOP in the eyes of RRD depends on the balance between aqueous production from the ciliary body and outflow through the trabecular meshwork and the bare retinal pigment epithelium. As the extent of retinal detachment with macular hole increases, the outflow through the retinal pigment epithelium may increase exponentially, resulting in hypotony and CD.
The identification of retinal breaks, especially of the macular hole, in eyes with CD may prove somewhat difficult as the result of aqueous flare, vitreous haze, and insufficient pupillary dilation. In this study, the macular hole was not preoperatively detected as the result of hazy media in 2 out of 4 cases of combined CD and RRD with macular hole. Preoperative suspicion and adequate surgical planning appears to be crucial in these cases, as RRD associated with macular hole tends to result in poor visual outcomes and a high incidence of redetachment.17,18 And, In the presence of macular hole with combined CD in RRD patients, pars plana vitrectomy should be contemplated.
In conclusion, the possibility of the presence of macular hole is to be taken into account preoperatively in cases of combined CD and RRD, particularly in cases in which marked hypotony is present in patients with high myopia.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






