Central Retinal Artery Occlusion Masquerading as Branch Retinal Artery Occlusion
Article information
Dear Editor,
Retinal artery occlusion (RAO) is characterized by attenuated arterioles and ischemic retinal opacity, which suggest retinal infarction. Branch RAO (BRAO) has a more favorable prognosis than central RAO (CRAO). CRAO and BRAO can be differentiated based on the ischemic retinal opacity area, location of the attenuated vessels, and a cherry-red spot [1]. However, we encountered a case of CRAO masquerading as BRAO and have reported this case with a review of the relevant literature.
An 81-year-old man complained of sudden visual disturbance in his right eye, which first appeared 2 days prior. The best-corrected visual acuity was hand motion. Sixty years prior, the patient's left eye had been enucleated due to ocular trauma. He was diagnosed with inferior BRAO in his right eye 6 years prior to presentation (Fig. 1A and 1B). Fundus photography revealed a supratemporal ischemic opacity without a cherry-red spot, which indicated superior BRAO (Fig. 1C). However, fluorescein angiography (FAG) showed non-arterial filling with CRAO (Fig. 1D), while brain angiography revealed internal carotid artery occlusion. The middle cerebral artery was supplied by collateral vessels in the anterior communicating artery and posterior communicating artery, but major collateral vessels in the ophthalmic artery were not identified.
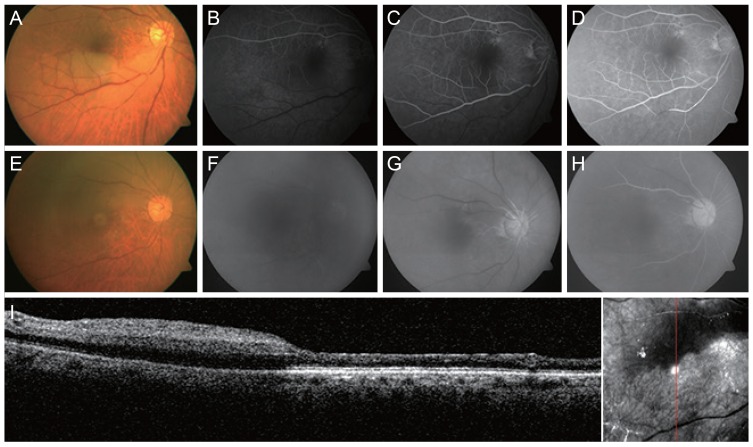
(A) Fundus photograph of branch retinal artery occlusion (RAO) with an ischemic opacity at the inferotemporal lesion 6 years before presentation. (B-D) Early-to-late phase fluorescein angiography of branch RAO with non-perfusion in the inferotemporal arcade 6 years before presentation. (E) Fundus photograph of the recent central RAO with an ischemic opacity in the superior retina. (F-H) Early-to-late phase fluorescein angiography of the recent central RAO with blockage of the whole retinal artery. (I) Vertical view of spectral domain optical coherence tomography revealed an edematous retina with an ischemic opacity lesion and without any edema change in the existing branch RAO lesion.
In the current case, CRAO in a patient with a previous history of BRAO mimicked BRAO, because the previously BRAO-effected retina did not exhibit an ischemic retinal opacity during fundus examination.
Retinas with BRAO or CRAO normally display a retinal ischemic opacity lesion. This irreversible damage to the inner and outer retina is finally atrophied [2]. Opacity lesions are more prominent in the posterior pole with more than one ganglion cell layer, because these lesions may result from opacification of the retinal ganglion cells caused by acute ischemia. For the same reason, the peripheral retina with a single layer of ganglion cells or atrophic retina with damaged ganglion cells does not exhibit a distinct retinal opacity in acute arterial occlusion. Hayreh [3] suggested that CRAO lasting for approximately 240 minutes can lead to irreversible retinal damage in Rhesus monkeys. Optical coherence tomography and histologic examination revealed that irreversible retinal damage may be specifically due to thinning of the inner retina. Thinning of the retina indicates retinal damage [24]. In the present case, the inferior retina appeared to be intact despite FAG findings of CRAO because, with the exception of the atrophic retina where the previous inferior BRAO was observed, the superior retina was edematous and opacified (Fig. 1C-1I).
In conclusion, cases of CRAO with a history of BRAO may appear as BRAO when the non-perfusion of the previous BRAO lesion is masked. FAG should be performed and a detailed history should be taken for RAO diagnosis.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.