


Dear Editor,
Kelly and Wendel [1] first introduced vitrectomy to treat macular holes (MHs) in 1991, and Eckardt et al. [2] reported internal limiting membrane (ILM) peeling during MH surgery in 1997. Currently, the primary surgical treatments for MH are pars plana vitrectomy (PPV), ILM peeling, and gas tamponade. Although the primary hole closure rate reaches more than 90% with current methods, the failure rate is much higher in cases with high myopia, chronic MH, nonidiopathic condition or large MH, defined as a hole diameter bigger than 400 ╬╝m [3]. Recently, ChŌĆÖng et al. [4] reported a closure rate of 76% in MHs >650 ╬╝m. Various secondary surgical options have been proposed for recurrent and persistent MHs, such as additional ILM peeling, ILM flaps, and lens capsule transplantation [3]. Chen and Yang [5] demonstrated lens capsular flap transplantation to treat refractory MH and showed hole closure and visual improvement. Herein, we report a case of refractory large MH successfully treated with anterior capsular flap transplantation after a failed primary surgery. Informed consent for the publication of this case report and relevant images was obtained from the patient.
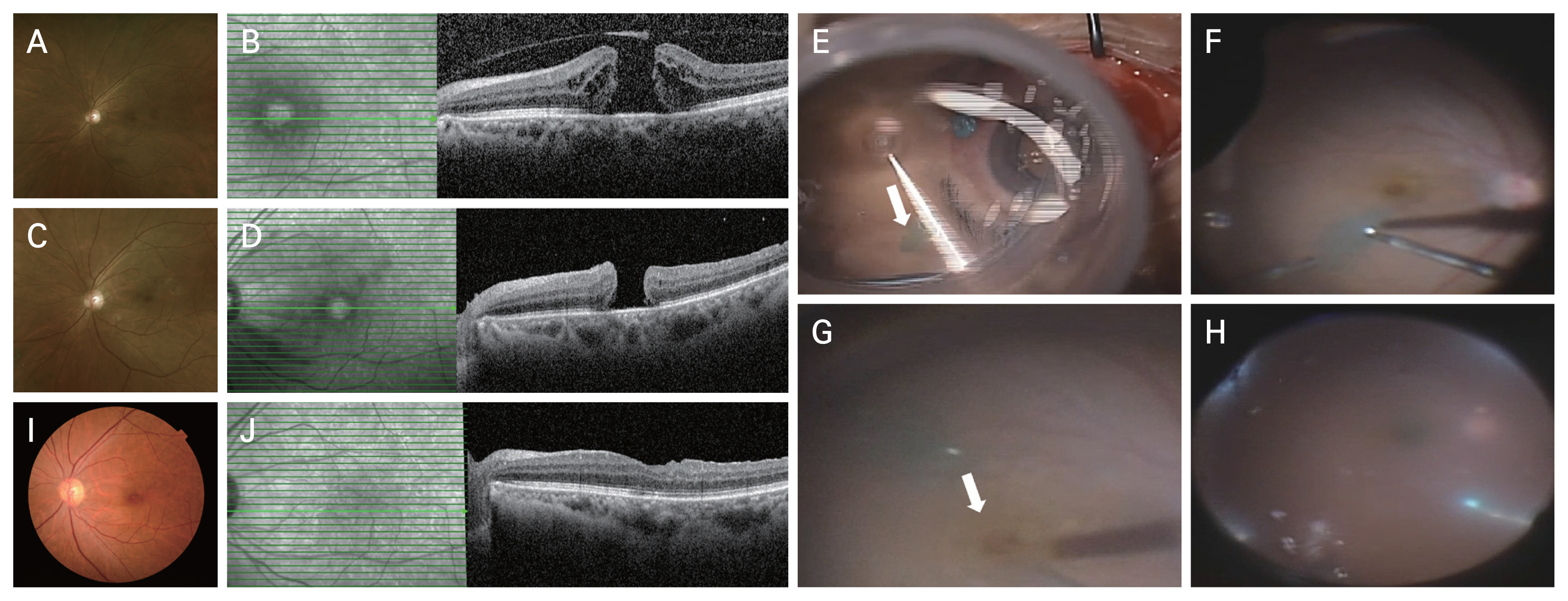
A 66-year-old female patient presented with metamorphopsia and decreased vision in her left eye for more than 1 week. She had well-controlled diabetes and hypertension as underlying diseases. Her best-corrected visual acuity (BCVA) was 20 / 20 in the right eye and 20 / 1,000 in the left eye. The intraocular pressure was 14 mmHg in both eyes. The anterior segment examination was unremarkable, and she had mild cataracts in both eyes. Fundus examination revealed full-thickness MH in the left eye (Fig. 1A). On optical coherence tomography (OCT) scans, the MH size was 694 ╬╝m at the minimal diameter and 1,276 ╬╝m at the base diameter (Fig. 1B). To treat a large MH, PPV, ILM peeling, and intravitreal injection of 10% perfluoropropane were performed under local anesthesia by KWB. During the operation, the ILM was stained with 0.05% indocyanine green (Pulsion Medical Systems AG) and was widely removed up to the major arcades. Postoperatively, we recommended maintaining the head-down position for 1 week. One month postoperatively, the MH was still not closed (Fig. 1C, 1D), and a second operation was conducted after a thorough and careful discussion with the patient. We considered autologous anterior capsular flap transplantation to close the refractory MH. Under local anesthesia, phacoemulsification and posterior chamber intraocular lens insertion was first performed. An anterior capsule flap was obtained during cataract extraction (Fig. 1E) and introduced into the vitreous cavity by ILM forceps (Fig. 1F). While positioning the capsular graft on the MH, the infusion was temporarily turned off to ensure that the flap did not dislocate from the intended position. In addition, a small amount of DisCoVisc (hyaluronic acid 1.6%-chondroitin sulfate 4.0%, Alcon Laboratories) was injected around the MH to secure the graft in place (Fig. 1G). After transplantation, fluid-air exchange was carefully performed to avoid displacing the flap until the end of the operation (Fig. 1H). Finally, surgery was completed after an intravitreal injection of 14% perfluoropropane (Supplementary Video 1). Postoperatively, the patient was asked to maintain a head-down position for 1 week. Complete hole closure was validated by OCT scans 1 month after the second operation (Fig. 1I, 1J). Three months after the capsule graft operation, her BCVA improved to 20 / 40 in the left eye, and the MH remained closed. Notably, significant recovery of the outer retinal layer of the fovea, including the external limiting membrane, ellipsoid zone, and interdigitation zone, was observed on the OCT images.
In conclusion, we reported a case of refractory large MH that was successfully treated with anterior capsule flap transplantation. To the best of our knowledge, this is the first report of a refractory large MH successfully treated with reoperation using an anterior lens capsule graft in Korea. Our case suggests that despite initial surgical failure, subsequent intervention has the potential to yield anatomically and functionally satisfactory improvement, thereby offering a favorable prognosis. Autologous anterior capsular flap transplantation is an effective treatment option for refractory MH.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement
Supplement Print
Print






