

Dear Editor,
Giant cell arteritis (GCA), also known as temporal arteritis, is a systemic autoimmune disease primarily affecting the elderly. It is characterized by granulomatous inflammation of large and medium-sized arteries [1]. Arteritic anterior ischemic optic neuropathy (AAION) is the most common type of ophthalmic complication of GCA, and can cause permanent visual loss [2]. Therefore, AAION represents a true ophthalmic emergency, because the possibility of visual loss is very high if it is not recognized and treated promptly [3]. There have been few reports of GCA among Asians, and only one involving a patient with silent GCA-associated AAION in Korea [2]. Herein, we report a case of GCA-associated AAION with typical systemic GCA symptoms in an elderly Korean man, as confirmed by temporal artery biopsy.
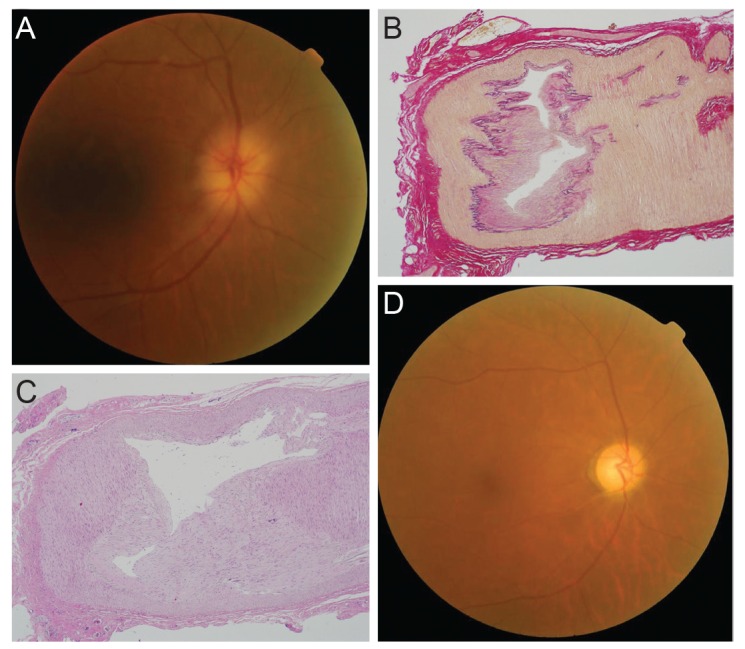
A 70-year-old man presented with sudden vision loss in his right eye (oculus dexter, OD), which had occurred the previous day. He had been suffering headaches for several months, and anorexia, general weakness and scalp tenderness were also noted during this period. His best-corrected visual acuity (VA) was 10 / 20 in OD and 20 / 20 in the left eye (oculus sinister, OS). A relative afferent pupillary defect was also noted in OD and intraocular pressure was 14 mmHg in OD, 12 mmHg in OS. Both eyes were freely movable and non-tender upon eye movement. A chalky white swelling in OD was discovered upon fundus examination (Fig. 1A), and visual field testing (Humphrey HFA II; Carl Zeiss Meditec, Jena, Germany) revealed a near total field defect in the same eye. The Hardy-Rand-Rittler test showed total dyschromatopsia in OD and fluorescein angiography revealed delayed filling of the vertical watershed zone at the adjacent nasal peripapillary choroid and optic disc leakage at late phase. The patient's body temperature was 38.3Ōäā and white blood cell count was 12,900/mm3. C-reactive protein levels, as well as the erythrocyte sedimentation rate, were also elevated to be 14.5 mg/dL (upper normal limit, 0.5 mg/dL) and 108 mm/hr (upper normal limit, 20 mm/hr), respectively. The patient was admitted on the presumption of GCA with AAION, although we could not completely rule out systemic infection, because AAION is very rare in Korea. For this reason, we systematically evaluated potential foci of infection, and the patients was administered intravenous empirical antibiotics.
After 2 days, the patient's VA in OD had decreased to finger-count. Disc swelling remained, and a disc hemorrhage had newly developed. Computed tomography of the chest and abdomen revealed no definitive infection focus. We planned temporal artery ultrasonography and biopsy, and the patient was referred to the Department of Rheumatology.
On hospital day 5, temporal artery ultrasonography revealed no evidence of temporal arteritis. The intravenous antibiotics were stopped, and a once-daily course of intravenous methylprednisolone (62.5 mg) was started. A biopsy was performed at the right temporal artery. It showed an intimal thickening and inflammatory cells within the media of arterial wall (Fig. 1B and 1C). GCA was thereby confirmed and intravenous steroid therapy was maintained. The C-reactive protein and erythrocyte sedimentation rate level had both decreased after 3 days of steroid treatment, to 2.86 mg/dL and 79 mm/hr, respectively.
On hospital day 13, the patient's VA OD had improved to 6 / 20, and disc swelling had decreased. His general condition had also improved. Oral prednisolone therapy was slowly tapered from 60 mg per day to 15 mg per day. However, after 1 month, the patient's VA OD had decreased to 3 / 20, and visual field testing showed a progressed visual field defect. What is more, pale optic disc in OD was found upon fundus examination (Fig. 1D). Optical coherence tomography revealed decreased macular ganglion cell layer thickness in OD. OS had not been affected.
In summary, we presents a case of AAION with typical systemic symptoms of GCA and pathological findings of diffuse inflammatory cell infiltration of the temporal artery in an elderly Korean man. To our knowledge, there has only been one other report of a biopsy confirmed case of GCA-related AAION in Korea [2]. However, unlike our patient, the previous report involve silent GCA with no systemic symptoms. Therefore, this is the first biopsy confirmed report of GCA-associated AAION with typical systemic symptoms of GCA in Korea.
In conclusion, although GCA-associated AAION is very rare in Koreans, it can indeed occur. A rapid diagnostic work-up involving erythrocyte sedimentation rate, C-reactive protein and temporal artery biopsy, as well as prompt corticosteroid treatment, may be necessary to save the vision in the affected eye, and to prevent the involvement of the other eye.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






