

Amblyopia is defined as decreased visual acuity in patients with strabismus, anisometropia, or pattern vision deprivation and has an onset during visual immaturity [1]. A dioptric difference between the eyes is one of the most common causes of amblyopia. If a retinal image is blurry in one eye, then the visual acuity of the other eye cannot develop properly. The retinal image of the fixed object is unclear in the eye with the more severe refractive error, particularly when children develop anisometropia. The visual stimulus is thus insufficient for proper development of visual acuity. Therefore, correction with spectacles or occlusion therapy is used to treat amblyopia [2]. Amblyopia treatment techniques exhibit diverse outcomes, which vary based on the initial cause, degree of disease, age at the start of amblyopia treatment, and patient compliance. Although the definition of success for amblyopia varies, up to 75% of patients improve with treatment [3]. In a retrospective study of 163 children with pure anisometropic amblyopia, Woodruff et al. [4] reported that approximately 60% of patients achieved a final visual acuity of 6 / 9 or better. However, amblyopia treatment may still fail despite appropriate amblyopia treatments.
Higher-order aberration (HOA) is a known index of visual quality. When ocular (global) aberrations increase during development, visual symptoms can occur, such glare, halo, and distortion. Some studies have reported that correcting HOAs can significantly improve visual acuity. Yoon and Williams [5] reported that HOA correction improved contrast sensitivity and visual acuity and Rossi et al. [6] reported that even cases of emmetropia and low myopia would benefit from HOA correction. Therefore, HOAs could affect the results of amblyopia treatment. However, little is known about the relationship between HOAs and amblyopia treatment.
The KR-1W aberrometer (Topcon Medical System, Tokyo, Japan) measures the development of total ocular aberrations using ocular aberrometry and corneal topography simultaneously [7]. Internal aberrations produced by the lens can be calculated easily from this information by subtracting the corneal aberrations from total ocular aberrations. The advantages of this calculation include always using the same reference axis, thereby avoiding errors caused by misalignments when measuring corneal and ocular wavefront profiles. As a result, ocular, corneal, and internal HOAs can be obtained simultaneously. In addition, this procedure has been reported to have a relatively high intra-subject repeatability [7]. Therefore, in this study, we investigated the relationship between HOAs and amblyopia treatment using a KR-1W aberrometer in children with hyperopic anisometropic amblyopia.
Materials and Methods
We retrospectively reviewed the medical records of amblyopia patients treated from February 2011 to January 2013 in the Pediatric Ophthalmology Clinic at the Inje University Ilsan Paik Hospital. Clinical data included patient age at initial visit, gender, uncorrected visual acuity (UCVA), best-corrected visual acuity (BCVA), alternate cover test, and slit-lamp and fundus examinations. We calculated the spherical equivalent (SE) according to the results of the cycloplegic refraction at the initial and follow-up visits.
The following inclusion criteria were applied: hyperopic anisometropic amblyopia, defined as bilateral hyperopia representing a difference in the SE between the eyes (spherical anisometropia) of 1.00 diopter (D) or more, a difference of at least two lines in the BCVA of both eyes using the Snellen visual acuity chart (Yong Han Jin chart), and a BCVA of 0.63 or better in the fellow eye when the patient was younger than 6 years or 0.8 or better in the fellow eye when the patient was aged 6 years or older. Patients with complete 12-month follow-up examinations and treatments were included in this study. The following exclusion criteria were applied: patients with an astigmatism of 1.00 D or more in the amblyopic eye, difference in the astigmatism between the eyes (astigmatic anisometropia) of 1.00 D or more, myopia, strabismus, abnormalities in the anterior segment of the eye or fundus, ocular diseases, ocular trauma, history of ocular surgery, history contact lens use, and history of amblyopia treatment.
Based on the degree of spherical anisometropia, subjects were categorized with mild, moderate, or severe hyperopic anisometropia. Patients with spherical anisometropia of at least 1.00 D but less than 2.00 D were classified with mild hyperopic anisometropia, patients with spherical anisometropia of at least 2.00 D but less than 3.00 D were classified with moderate hyperopic anisometropia, and patients with spherical anisometropia greater than 3.00 D were classified with severe hyperopic anisometropia.
Prescription spectacles that fully corrected the refractive error made after initial evaluation, BCVA measurement, and the confirmation of corrective compliance with spectacles were completed at the 1-month follow-up. Correction compliance using the spectacles was assessed according to parental and patient reports. Each day, the amount of time spent wearing the spectacles was recorded (excellent, all waking hours; fair, half or more of the waking hours; poor, less than half of the waking hours). Occlusion therapy was added if a difference of at least 2 lines between the BCVA of the eyes persisted full-time or part-time (4 to 6 hours per day) at the 3-month follow-up. Occlusion therapy compliance was assessed by parental and patient reports and the percentage of self-reported patching hours compared with the amount of prescribed patching hours were recorded (excellent, Ōēź80%; fair, Ōēź50% and <80%; and poor, <50%). Based on monitoring of the BCVA after 12 months of follow-up, results of amblyopia treatment were determined. Successful amblyopia treatment was defined as a difference of <2 lines between the BCVA of both eyes at any follow-up period and failed amblyopia treatment was defined as a remaining difference of Ōēź2 lines between the BCVA of both eyes after the 12-month follow-up.
HOAs were measured for all patients using a KR-1W aberrometer at the initial visit and at 3-month, 6-month, and 12-month follow-ups. HOAs were not measured at the 1-month follow-up. All HOA measurements were performed in a dark room and the patient was asked to blink once before the scan and focus on the fixation target before the scan was performed. Repeated HOA measurements were taken until the patient followed instructions. We chose the best scans using an unbroken Placido's disk and eye imaging obtained when the eye was uncovered by the eyelid. Then, the HOAs were analyzed using root mean square (RMS) values. Optical instability increased with greater RMS values. The HOAs were measured from three compartments: ocular, corneal, and internal HOAs. Total HOAs, trefoil, coma, and spherical aberration were obtained from each compartment with a 4.0-mm pupil.
Statistical analysis was performed with the SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). The Wilcoxon's signed-rank test was used to compare the measurements within each group, The Mann-Whitney U-test was used to compare the between-group measurements. Logistic regression was performed to evaluate the prognostic factors associated with the results of amblyopia treatment. Age at initial visit, initial BCVA, value of spherical anisometropia, spectacles correction compliance, occlusion therapy compliance, and RMS values of all HOAs were used in the analysis. A p < 0.05 was considered statistically significant.
Results
A total of 61 (66.3%) out of 92 hyperopic anisometropic amblyopia patients who fulfilled the study criteria cooperated with the KR-1W examination. Additionally, 16 (26.2%) out of 61 patients were excluded in this study because they were lost to follow-up. Therefore, 45 subjects were included in this study. All subjects attended every follow-up, including the initial visit and the 1-month, 3-month, 6-month, and 12-month follow-ups. The mean age at the initial visit of the 21 males and 24 females was 70.3 months (range, 45 to 172 months) (Table 1). Amblyopia treatment succeeded in 28 patients (62.2%, the success group) and failed in 17 patients (37.8%, failure group) after 12 months of treatment. There were no statistically significant differences between success and failure groups in terms of age, UCVA of the amblyopic eyes, BCVA of the amblyopic eyes, SE, astigmatism, spherical anisometropia, or astigmatic anisometropia at the initial visit (p > 0.05).
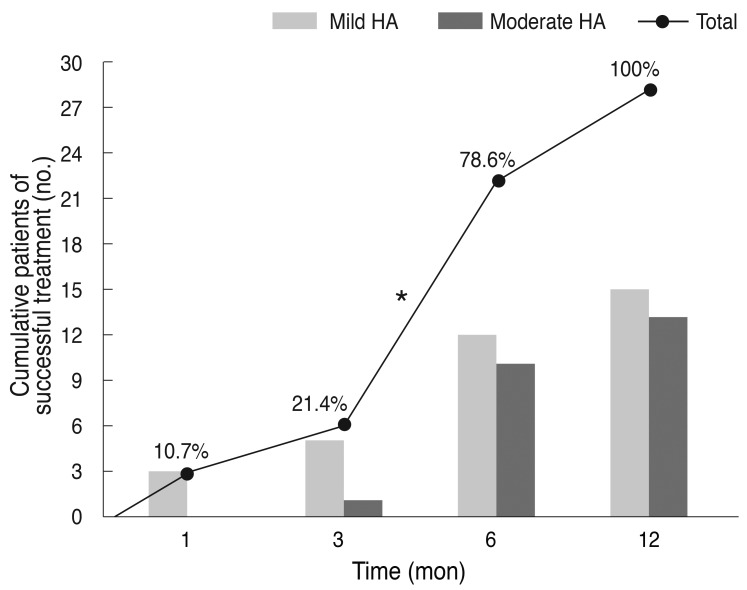
Mild hyperopic anisometropia was identified in 24 patients (53.3%) and 21 (46.7%) had moderate hyperopic anisometropia (Table 2). However, there were no severe cases of hyperopic anisometropia. For cases of mild hyperopic anisometropia, 15 patients (62.5%) were included in the success group and for cases of moderate hyperopic anisometropia, 13 patients (61.9%) were included in the success group. There was no statistically significant difference in the success rate between mild and moderate hyperopic anisometropia (p > 0.05). In the success group (28 patients), 16 patients (57.1%) succeeded in their amblyopia treatments between the 3-month and 6-month follow-up visits. This follow-up period had the highest success rate of all follow-up periods for both mild and moderate cases of hyperopic anisometropia (Fig. 1).
All 45 subjects received prescriptions for spectacles, and all of their compliances were recorded as 'excellent' (31 patients) or 'fair' (14 patients) at the 1-month follow-up. At the 1-month follow-up, three patients entered the success group and all patients had mild hyperopic anisometropia. A total of six patients received corrective spectacles only for use during the entire follow-up period. There were 10 full-time and 29 part-time occlusion therapy patients, and there were six full-time patients (60.0%) and 16 part-time patients (55.2%) in the success group. There were no statistically significant differences in the success rates between patients undergoing full-time or part-time occlusion therapy (p > 0.05). Of all patients who used occlusion therapy (39 patients), 12 patients had 'excellent' (30.8%) compliance, 25 patients had 'fair' (64.1%) compliance, and two patients had 'poor' (5.1%) compliance. Both of the patients who were rated as 'poor' compliance received full-time occlusion therapy and had moderate hyperopic anisometropia in the failure group. The subjects did not receive other amblyopia treatments other than corrective spectacles and occlusion therapy. Among all subjects, the mean pupil diameter was 5.02 mm (┬▒0.17; range, 4.67 to 5.32 mm) when measuring HOAs and there were no significant differences between the success and failure groups (p > 0.05).
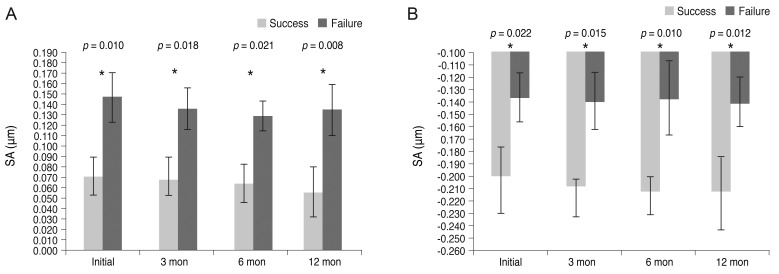
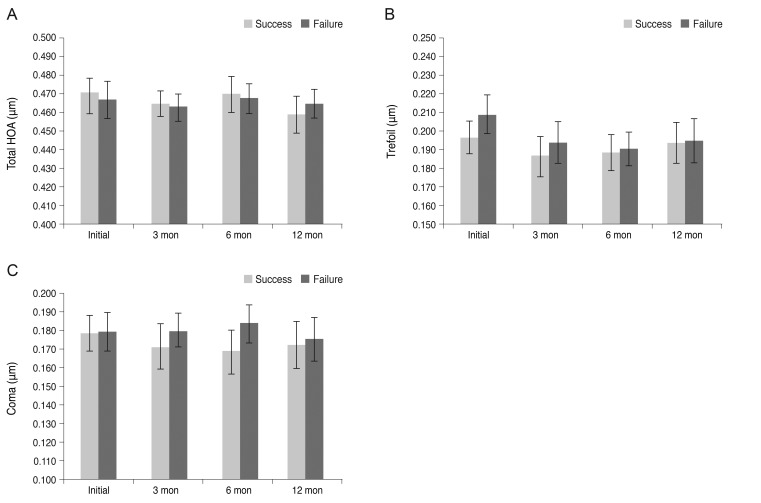
When comparing the two groups, the ocular spherical aberrations and internal spherical aberrations of the amblyopic eyes were significantly higher in the failure group at every follow-up (p < 0.05) (Fig. 2). There were no significant changes in the HOAs within the groups according to the follow-up data (p > 0.05). Furthermore, there were no significant differences in the total ocular HOAs, trefoil, or coma of the amblyopic eyes between the success and failure groups (p > 0.05) (Fig. 3). There were also no significant differences in the internal total HOAs, trefoil, coma, or corneal HOAs of the amblyopic eyes between the success and failure groups (p > 0.05).
There were no significant differences in the HOAs between patients with mild or moderate hyperopic anisometropia at any of the follow-up visits (p > 0.05). Ocular spherical aberrations and internal spherical aberrations of amblyopic eyes were significantly higher in the failure group than in the success group at every follow-up visit for both mild hyperopic and moderate hyperopic anisometropia (p < 0.05).
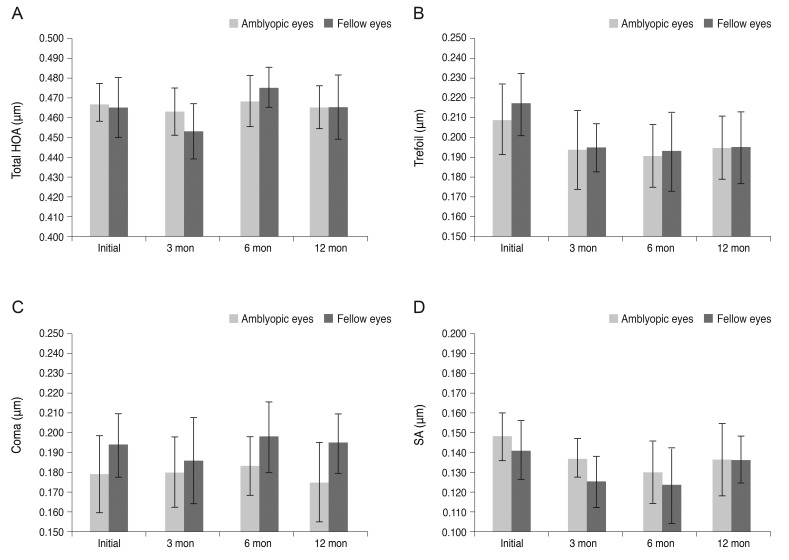
In the failure group, there were no significant differences in the total ocular HOAs, trefoil, coma, or spherical aberration between the amblyopic eyes and fellow eyes (p > 0.05) (Fig. 4). Furthermore, there were no significant differences in the corneal or internal HOAs between the amblyopic and fellow eyes (p > 0.05). In the success group, as in the failure group, there were no significant differences in the HOAs between the amblyopic and fellow eyes (p > 0.05).
Upon univariate logistic regression analysis, the RMS values of the ocular and internal spherical aberrations showed statistical significance with the results of the amblyopia treatment (p = 0.006 and 0.005, respectively). However, upon multivariate logistic regression analysis, the RMS values of the ocular and internal spherical aberrations showed no statistically significant differences for the results of amblyopia treatment.
Discussion
It is known that anisometropic amblyopia has an estimated prevalence in the pediatric population that ranges from 2% to 5% [8,9]. As a rule, amblyopia is more common and of a higher degree in patients with hyperopic anisometropia than in patients with myopic anisometropia [1,10]. Therefore, this study included only cases of hyperopic anisometropic amblyopia, which is the most common and severe form of amblyopia.
Weakley [11] reported thresholds for amblyopia development according to the type of anisometropia. In that study, thresholds included 1.00 D for hyperopic anisometropia, 2.00 D for myopic anisometropia, and 1.50 D for astigmatic anisometropia. They also reported that increasing levels of anisometropia beyond the thresholds resulted in an increased incidence and severity of amblyopia. Based on that report, this study included pure hyperopic anisometropic amblyopia patients with an astigmatism of <1.00 D in the amblyopic eye, spherical anisometropia Ōēź1.00 D, and astigmatic anisometropia of <1.00 D. To investigate the relationship between the degree of spherical anisometropia and the effect of HOAs on amblyopia treatment, subjects were categorized with mild, moderate, or severe hyperopic anisometropia. As a result, all hyperopic anisometropia patients with both spherical anisometropia Ōēź1.00 D or more and <3.00 D were included because there was no case of spherical anisometropia Ōēź3.00 D (severe hyperopic anisometropia). Therefore, this study was able to decrease the effects of lower-order aberrations (LOAs), which are composed of defocus (myopia, hyperopia) and astigmatism, in amblyopia treatment. No significant difference was found in the mean SE or in the value of spherical anisometropia between success and failure groups. There was also no significant difference in the success rate of amblyopia treatment according to the degree of hyperopic anisometropia.
Hussein et al. [12] reported that eyes with poor initial visual acuity and the presence of a significant astigmatism were less likely to achieve successful outcomes in cases of anisometropic amblyopia. However, this study was also unaffected by these risk factors. Because this study showed no significant differences in initial visual acuity between the success and failure groups, and initial astigmatisms were limited.
In anisometropic amblyopia, visual acuity is expected to improve after correction with spectacles alone. However, additional occlusion therapies may be more effective when amblyopia is not ameliorated after correcting with spectacles only. One study reported that occlusion therapy should be performed after using corrective spectacles for at least 16 weeks [13,14]. In this study, all subjects were prescribed spectacles only at the initial visit and additional occlusion therapy was performed when amblyopia was not treated by the 3-month follow-up. Woodruff et al. [4] reported that occlusion therapy had its maximum effect between 3 and 6 months. In this study, occlusion therapy almost certainly had its maximum effect before the 12-month follow-up, as occlusion therapy was initiated at the 3-month follow-up. Subjects had unequal occlusion times because this study was retrospective, however, there was no significant differences in success rates of amblyopia treatment between full-time and part-time subjects. However, because good compliance is necessary for successful occlusion therapy, we made an attempt to increase patient compliance. Several studies have reported that the compliance level of successful occlusion therapy ranged from 35% to 96% [15-17]. In this study, 12 of 39 patients (30.8%) had a compliance level Ōēź80%, while the compliance of 25 patients (64.1%) ranged between 50% and 80%. Thus, 37 patients (94.1%) recorded a compliance of 50% or more. Therefore, it is thought that the effect of amblyopia treatment on occlusion therapy compliance did not differ greatly from that of the success and failure groups. As a result, other causes that may affect amblyopia treatment were excluded as much as possible and thus, the study was well designed to evaluate the effect of HOAs.
Aberrations may be subdivided into LOAs, which can be corrected by spherocylindrical lenses, and HOAs, which cannot [18]. In terms of the quality of retinal images, 10% represented a combination of the effects of the HOAs, such as trefoil, coma, and spherical aberrations [19].
Recently, there have been a few reports about the relationships between HOAs and amblyopia. Prakash et al. [20] reported a single case of asymmetric HOAs and wavefront profiles measured using a Zyoptix workstation (Bausch and Lomb, Rochester, NY, USA) that possibly led to unilateral amblyopia. Then, Prakash et al. [21] studied 17 children with idiopathic amblyopia through follow-up lasting greater than 6 months and measured HOAs using a Zyoptix workstation wavefront analyzer. The authors reported that there were significant differences in the coma-like and trefoil-like aberrations between amblyopic and fellow eyes. They also concluded that it seemed highly likely for a subset of 'idiopathic' amblyopia to be associated with a loss of symmetry in the wavefront patterns between the two eyes. Zhao et al. [22] studied 38 children with refractory amblyopia over 32 months using a WaveScan Wavefront System (VISX, Santa Clara, CA, USA) aberrometer to measure HOAs. They reported that although LOAs were major factors determining retinal image quality, the HOAs also needed to be considered in amblyopic eyes as their effects were significant. Plech et al. [23] studied a group of patients who developed a total of 47 unilateral or bilateral cases of amblyopia over 1 year and measured the HOAs using an EyeTop2005 (CSO, Firenze, Italy). The authors reported that HOAs could have a bilateral amblyogenic effect when isometropia was present. However, Kirwan and O'Keefe [18] studied 30 children with strabismic and anisometropic amblyopia using an iTrace visual function analyzer to measure the HOAs (Tracey Technologies, Houston, TX, USA). They reported that the HOAs were similar in strabismic or anisometropic amblyopic eyes and in normal fellow eyes, however, unlike the LOAs, HOAs were unlikely to play a role in the development of amblyopia. Although these reports exist, conclusions of each report are difficult to align and it remains unclear how to best understand the relationship between HOAs and amblyopia/amblyopia treatment. In addition, spherical aberrations were not specifically reported in previous studies as compared to this study.
In this study, ocular spherical and internal spherical aberrations of amblyopic eyes were significantly higher in the failure group than in the success group at every follow-up. In light of these results, the failure group seemed to be more unstable in its optical aspect than the success group. However, there is no threshold that can absolutely judge HOAs.
In 1801, Young [24] described an instrument that could demonstrate the existence of a spherical aberration. A corneal spherical aberration typically exhibits +0.27 ┬Ąm on average and displays little or no relationship to aging [25-27]. In addition, the natural human lens typically exhibits negative spherical aberrations, which could result in reduced vision quality if not counteracted by the positive spherical aberration generally measured in the cornea [28,29]. The increase in internal spherical aberrations resulted in an increase of ocular spherical aberrations. In young, healthy people, corneal aberrations are almost completely compensated for by internal aberrations. There have even been some suggestions that the spherical aberrations at present could benefit our natural vision through improved depth of focus.
There have been no studies in children with high ocular spherical aberrations, particularly those with more internal spherical aberrations. Therefore, structural changes of the crystalline lens shape, as well as the gradient refractive index, may affect internal spherical aberrations in children and should be studied in the future [30]. Furthermore, there were no significant differences in the ocular spherical aberration or internal spherical aberration between the amblyopic and fellow eyes at any of the follow-up appointments. Therefore, we believe that spherical aberrations only affect the visual development of an eye with poor visual acuity, such as an amblyopic eye. However, a detailed study on this mechanism will be needed in the future.
For visual improvement beyond the typical territory of LOAs, optical and surgical treatments that can correct HOAs include adaptive optics [31], phase plates [32], customized soft contact lenses [33], and laser refractive surgery [34]. However, in reality, most of these methods for HOA correction are almost impractical in children because they are difficult to perform in this patient population. Thus, pediatric HOA corrections will be a topic greatly discussed in the future, even if some studies simply prove the obvious causality between HOAs and amblyopia treatment.
In conclusion, ocular spherical and internal spherical aberrations were significantly higher in children included in the failed amblyopia treatment group compared to children in the successful amblyopia treatment group. This finding suggests that in the amblyopic eye of hyperopic anisometropic amblyopia cases, higher ocular spherical aberration values result from a higher internal spherical aberration value, a characteristic among patients who failed amblyopia treatment. Therefore, HOAs, particularly ocular spherical and internal spherical aberration, should be considered as a reason for amblyopia treatment failure. The main limitation of this study is that there was no comparison to children without amblyopia. However, despite this limitation, this study was analyzed by properly controlling for other factors in accordance with restricted criteria and there are few previous reports on this topic. In this study, spherical aberration was primarily addressed in amblyopia treatment for the first time. However, more large-scale, long-term, and prospective research is needed to fully understand the relationship between HOAs, including spherical aberration, and amblyopia treatment.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






