

Although modern cataract surgery produces excellent clinical results, presbyopia-related issues remain. Although multi-focal intraocular lenses (IOLs), accommodative IOLs, and monovision are utilized to resolve presbyopia, they are imperfect solutions. Presbyopia is a state wherein the accommodative capacity of the lens is significantly diminished or lost completely. A known determinative mechanism for accommodation is the contraction of the circular muscles. When the circular muscles and longitudinal muscles of the ciliary body undergo antagonism and the longitudinal muscles relax, the contraction of the circular muscles (if they contract) act as a force and tend to reduce the diameter of the lens [1,2,3]. The power of the lens is enhanced as its elasticity transforms it into a convex shape. However, with the aging process, that elasticity usually degrades and the contractile force of the ciliary muscles, accordingly, abates. This in turn diminishes accommodative capacity, thereby causing presbyopia.
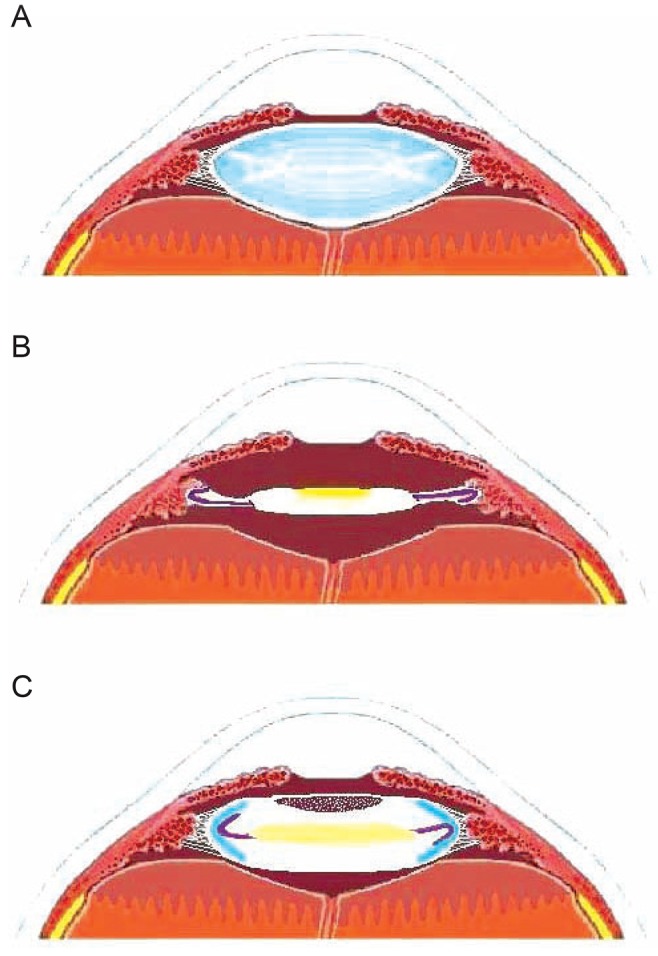
Accommodation is affected by the ciliary muscles' zonule, which is attached to the lens angle at the equator of the lens (Fig. 1A). Unfortunately, current cataract surgeries irreversibly reform the lens angle, resulting in the loss of accommodative capacity (Fig. 1B). However regardless of how old one becomes, the contractile force of the ciliary body continues to remain significant. Therefore, provided that the lens angle can be perfectly preserved, restoration of an infant-level accommodative capacity (over +50 diopters) is possible in place of a stiff crystalline lens by implanting an accommodative IOL optic that has one-tenth the volume of a stiff crystalline lens and the fluidity of an infant's lens.
The authors have called the process of lens-angle restoration during cataract surgery, 'lens-angle reconstruction (LAR)', the process for which they developed the lens-angle supporter (LAS). The authors expect to restore accommodative capacity by inserting IOLs while maintaining, by post-phacoemulsification LAS insertion, the normal structure of the lens angle (Fig. 1C).
This study evaluated LAS stability by means of a comparison of IOL location, after-cataract and ciliary body damage after cataract surgery in two groups of rabbits: experimental rabbits implanted with both the LAS and IOL after phacoemulsification (no. 5, 6, 7, and 8 rabbits) and control rabbits implanted with only the IOL (no. 1, 2, 3, and 4 rabbits).
Materials and Methods
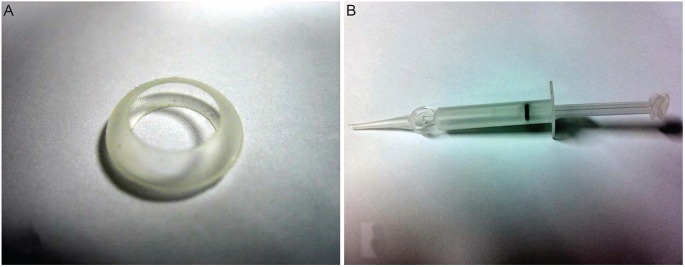
Animal experiments were conducted in compliance with the statement of the Association for Research in Vision and Ophthalmology regarding the use of animals in ophthalmic and vision research. The animals (8 rabbits aged over 1 year) were raised in comfortable cages and provided with nutritious food. Prior to surgery or examination (both performed by a skilled surgeon), suffering was ameliorated by anesthetic drugs (zolazepam 15 mg/kg, xylazine 5 mg/kg) and an anti-inflammatory drug (ketoprofen 5 mg/kg). After deep anesthetization, the animals were sacrificed using an intravenous potassium chloride overdose. This study used the LAS, a device developed by the authors (Fig. 2A). The LAS is made of silicone elastomer and has a 9.0 to 12.0 mm diameter formed in 0.1 mm increments. Its thickness is 227 to 298 ┬Ąm. The LAS can be folded so that it can be implanted through a 3.0 mm corneal incision and its excellent restorative force allows it to maintain its shape once implanted into the capsular bag. The authors also developed an injector for LAS implantation (Fig. 2B). Using this injector, the LAS can be easily implanted through the 3.0 mm incision. We obtained LAS samples from the LOSEC Corporation (Seoul, Korea), which had obtained Korean Food and Drug Administration approval for LAS use in animals.
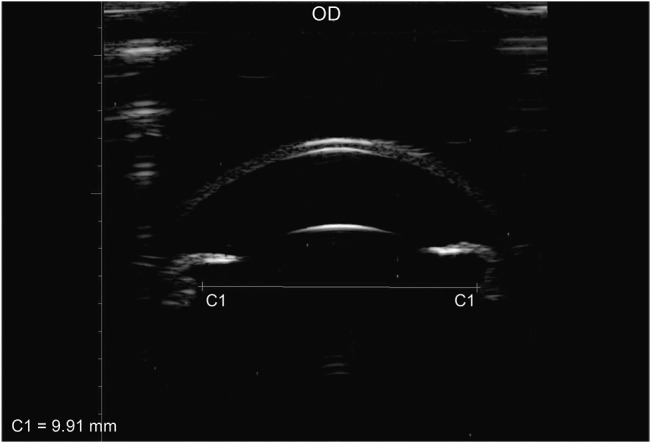
The size of the lens was measured using an ultrasound biomicroscope (UBM; AVISO, Quantel Medical, Cedex, France) in order to determine the size of the LAS to be implanted [4,5]. Estimates of the lens size were obtained by measuring the ciliary process inner diameter via a 25 MHz or 35 MHz UBM after administering anesthesia to the rabbits to render them in a state of accommodation paralysis.
Although LAS size was determined using a UBM, the equator of the crystalline lens was not observed due to the iris. Additionally, the zonules were not observed in most cases. Instead, the inner distance between the ciliary processes was measured. For this, the 25 and 35 MHz UBM proved useful. A 20 MHz UBM displayed good permeability, although one disadvantage was the failure to clearly capture the entire eye. However, a 50 MHz UBM displayed good resolution for the iris and upper portion of the iris, but had insufficient permeability, causing the ciliary body to look relatively out of focus. For the further purposes of this study, the inner diameter of the ciliary processes was measured and for appropriate resolution and permeability, the 25 MHz UBM was used (Fig. 3).
The eight rabbits were divided into an experimental group of four rabbits and a control group of four rabbits. Surgery was carried out on the right eye only. Four sizes of LAS were determined by subtracting 0.3, 0.5, 0.7, and 0.9 mm from the ciliary process's inner diameter (IDCP). Following phacoemulsif ication and ir rigation and aspiration (I&A), the four LAS's and their corresponding IOLs were implanted into four experimental rabbits. For the four rabbits in the control group, only the IOL was implanted.
For surgery, rabbits were intravenously administered anesthesia. The nuclear remnants were removed as much as possible using a continuous curvilinear capsulorhexis (CCC) with a 4 to 5 mm opening that allowed sufficient time for phacoemulsification. Then the cortex was completely removed via I&A. Using the injector, the LAS was implanted, followed by its corresponding IOL (LI61AO +21.0 diopters; Baush & Lomb, Rochester, NY, USA). Corneal sutures were carried out once with 10-0 nylon. After the surgery, ofloxacin and ocumetholone eye drops were administered four times a day and 0.1% atropine was administered once a week for three months after surgery.
Six months af ter the surgery, the rabbits were intravenously administered anesthesia and then euthanized with a potassium chloride injection. Subsequently, the IOL location and condition of the lens capsule were determined using a slit-lamp examination. Following enucleation, the rabbit eyes were frozen with nitrogen at -80 degrees. The eyeball was then dissected at the equator and photographed in Miyake-Apple view, in preparation of an UBM examination of the IOL location, lens capsule condition and ciliary body [6].
Results
Experimental group
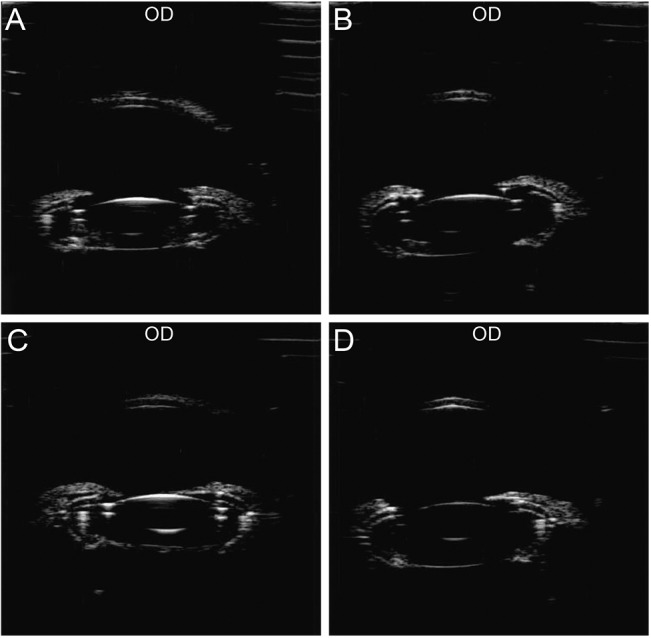
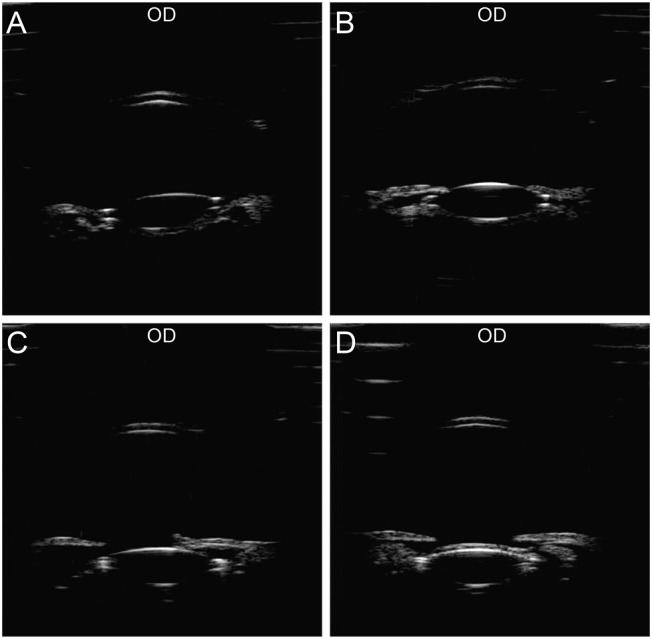
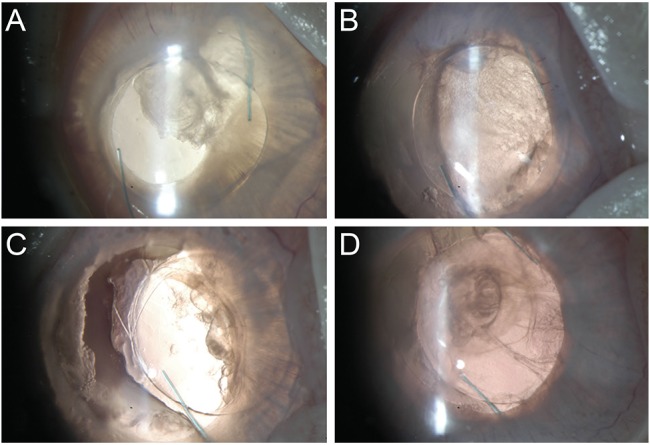
Based on the UBM results, the LAS and IOL showed normal positioning in all four cases. The lens angle was maintained and the posterior capsule was observed (Fig. 4). Based on the slit-lamp examination and Miyake-Apple view, the IOL was positioned at the center with less after-cataract and the ciliary body showed less damage (Figs. 5 and 6). Rabbit 5 showed the least extent of after-cataract with an intact ciliary body. Additionally, with regard to the severity of ciliary body damage and after-cataract, relatively more ciliary body damage and more severe aftercataract occurred with smaller-size LAS's.
The after-cataract in three of the four cases did not cover the visual axis. When an LAS of 0.1 mm smaller than the ciliary process inner diameter was implanted, the size of the LAS was too large to be properly unfolded. However, the authors were able to substitute a smaller LAS without any problems. There was no infection or any other complication in any of the cases. In conclusion, the most appropriate size of the LAS was determined to be 0.3 mm smaller than the ciliary process inner diameter during pupil dilation.
Control group
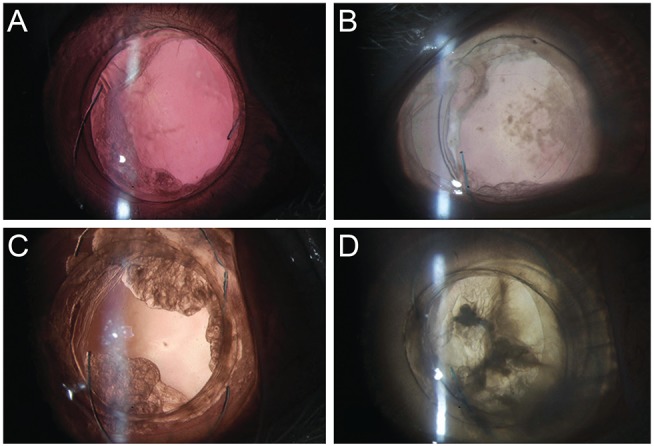
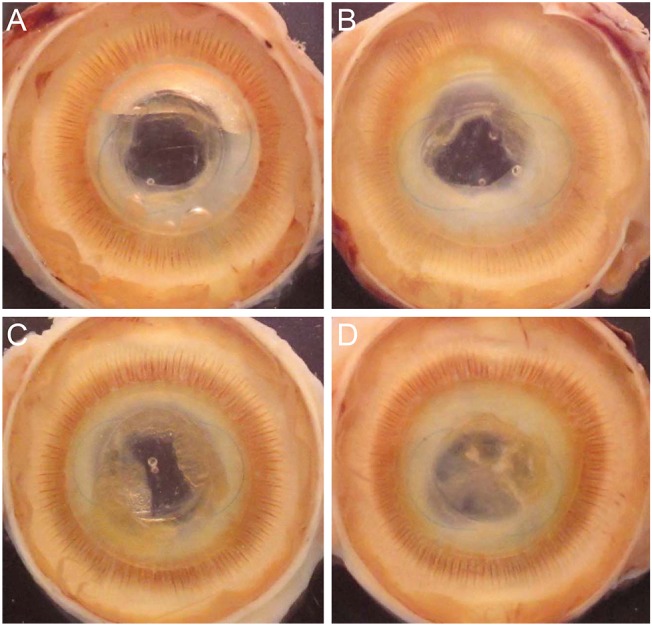
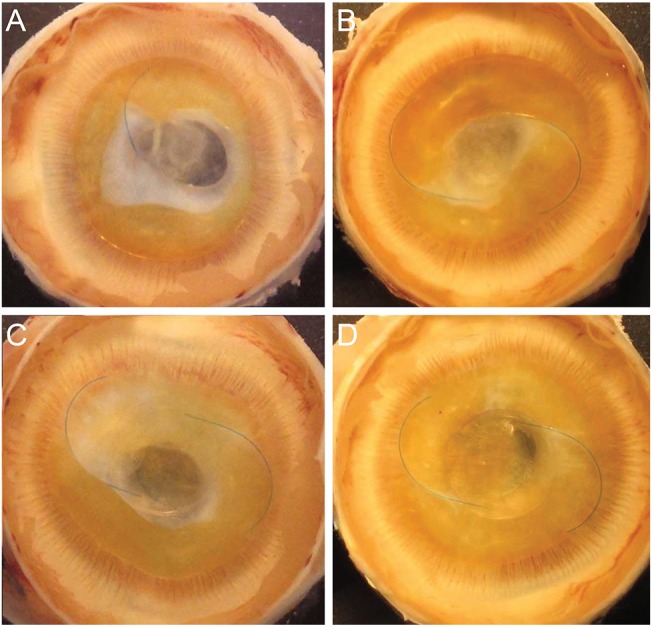
According to the UBM results, the experimental group (Fig. 4) showed consistent IOL positioning and the control group showed IOLs that were located in a higher position than the normal in two cases (Fig. 7A and 7B). There was also a single case where the IOL was decentered (Fig. 7C) and there was only one case which showed normal intraocular lens positioning (Fig. 7D). Lens angles were not maintained in all control cases. The following were the specific slit-lamp observations: haptic caused damage to the iris at the 1 o'clock location (Fig. 8A); slanted IOL optic (Fig. 8B); separated after-cataract mass that caused decentering of the IOL at a 3 o'clock location (Fig. 8C); a single case with normal intraocular lens positioning (Fig. 8D). In the Miyake-Apple view, most of the IOL haptics were protruding into the ciliary process (Fig. 9). Except for a single case (Fig. 9A) in which only one haptic was seen, all other cases showed a damaged ciliary body and expansion in the direction of the IOL haptic protrusion.
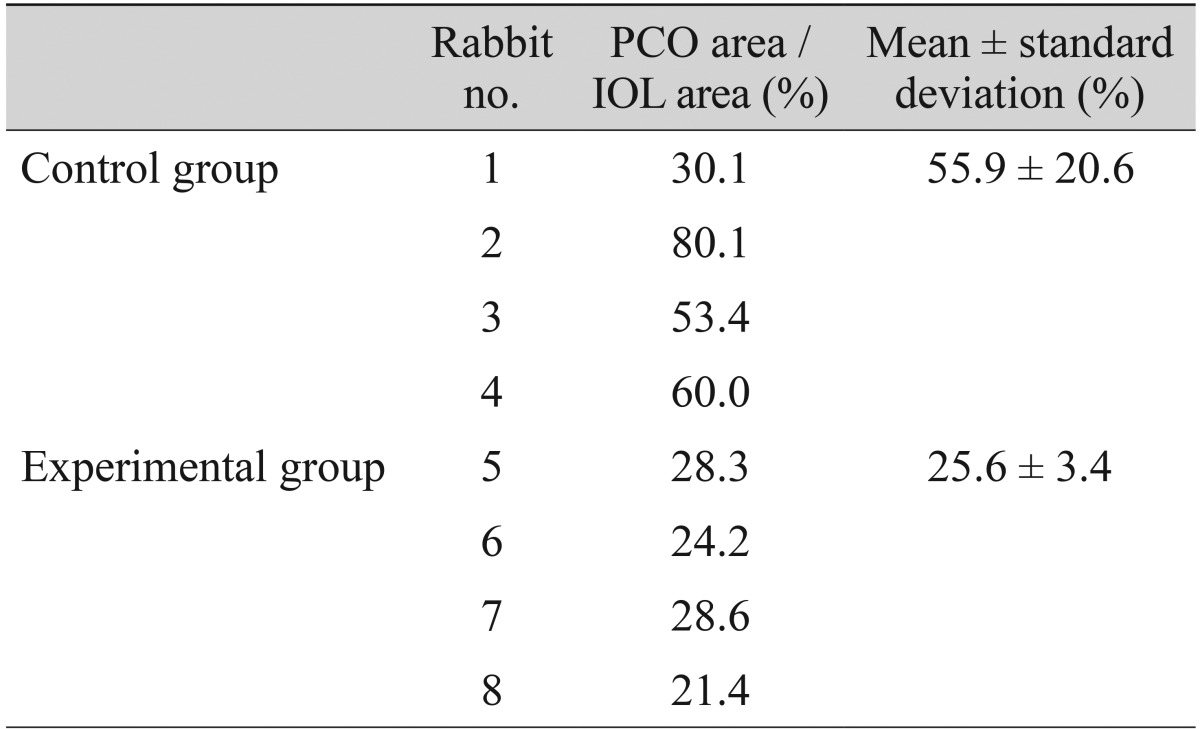
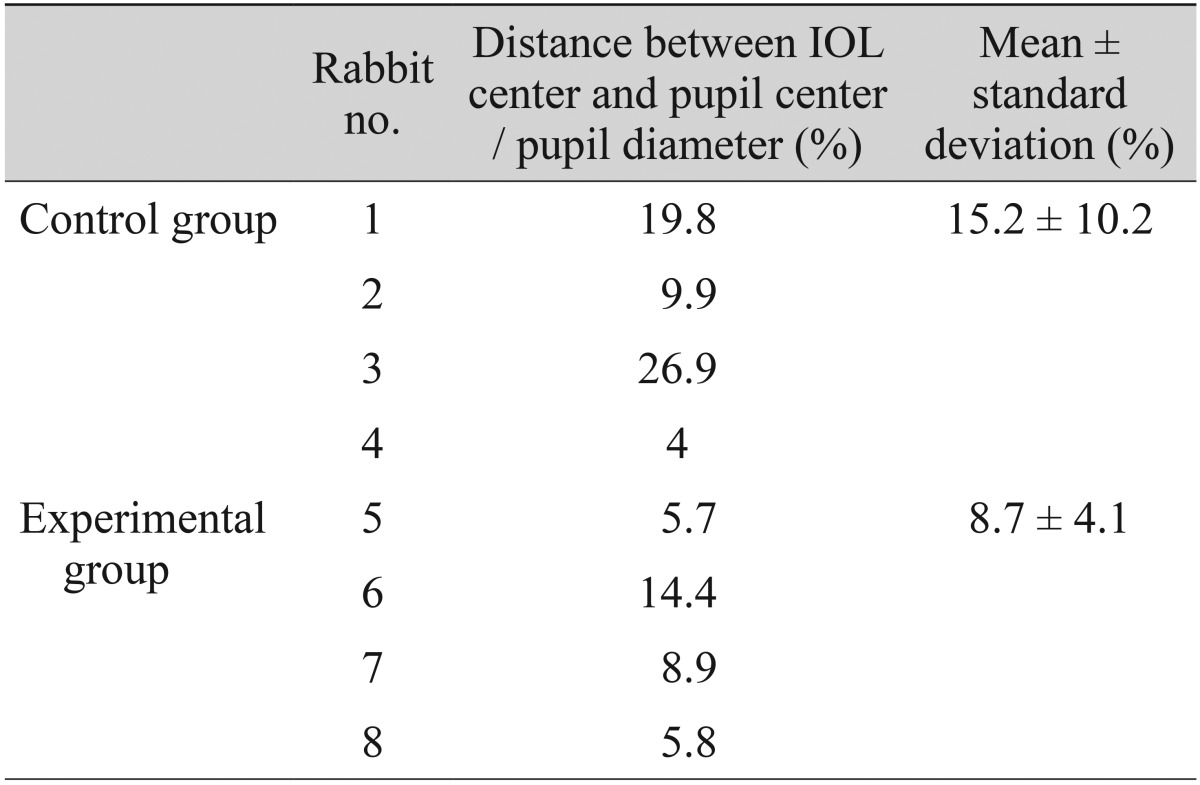
In all the control cases, after-cataract occurred more severely than in the experimental group. One case manifested the most severe after-cataract within the control group, despite good IOL positioning (Fig. 9D). The ratio of posterior capsular opacity area to IOL area was calculated in order to compare the amount of after-cataract in each group (Table 1) and the ratio of the distance between the IOL center and the pupil center to pupil diameter was calculated in order to compare the IOL centering in each group (Table 2).
Discussion
The reconstruction of the lens angle, which is irreversibly re-formed during the course of conventional cataract surgery, is the most critical element in achieving a perfectly functioning, accommodative IOL [7,8,9,10]. The objective of this study was to determine whether the lens angle could be recovered and the LAS positioned appropriately, without complication after LAS implantation. Silicone elastomer was used as the LAS material because it can be implanted into the eyeball in a folded state and has enough restorative force to recover its original shape without causing any foreign body reaction in a living body. Indeed, all of the above conditions were met in the experiment.
Eye-size consistency was the rationale for the use of rabbits more than 1 year old in the present study. In the case of rabbits that are still growing at less than 1 year old, eye size increases as weight increases, thereby increasing lens size, making accurate results difficult to achieve. Several limitations should be noted about the current study. First, the main challenge was the complete removal of the lens's nuclear remnants, which was accomplished successfully only by phacoemulsification, not I&A. The nuclear remnants, a syrup-like-, flexible-, and transparent fluid from the surgical view, evade the phaco tip, become mixed with the balanced salt solution, and spread to the inner capsular sac, iris and anterior chamber. Remnants have strong adhesive properties, which result in yellowish staining of the iris, IOL optic and haptics.
Due to the adhesion of the nuclear remnants, none of the eight eyes from either the experimental or control groups, reacted to the cycloplegics or miotics six months after the operation. Accordingly, the authors postponed the original plan to measure the experimental group's lens angle or change in LAS shape in a cycloplegic and miotic state using UBM. This will be undertaken in future clinical research. Second, using the LAS, we were able to successfully recover the lens angle and achieve stable positioning of the IOL, but could not measure the lens-angle curvature. If lens angle is important, its degree of angulation degree might be very important as well. Third, the IOL used in this study were designed for the human eye and thus was somewhat small for rabbits. Therefore, in order to establish the efficacy of the LAS for IOL decenteration, utilization of a larger IOL suitable for the rabbit eye, as a control, will be necessary. Fourth, because the anterior and posterior capsule did not adhere, after-cataract decreased significantly, though the IOL in the capsular bag might not have achieved firm fixation. Finally, the small sample size was another limitation to this study. All of these issues will have to be considered in future clinical research. These limitations notwithstanding, the LAR surgery carried out as part of this study successfully reconstructed the lens angle and there was no significant damage to the ciliary body in the process. Furthermore, by providing more stable support to the IOL haptic than is currently possible by conventional cataract surgery, consistently good positioning of the IOL was ensured. Additionally, as the anterior and posterior capsule never came into contact after surgery, after-cataract was significantly decreased. This indicates that LAR surgery provides a useful support not only for perfectly functioning accommodative IOL in correcting presbyopia, but also for general cataract surgery.
Even in cataract surgery with conventional artificial IOL implantation, if the LAS is implanted with the IOL, the IOL can be replaced at anytime. This is a key advantage because the lens angle can be preserved without being irreversibly reformed, thereby allowing for replacement of artificial IOLs with improved accommodative IOLs that will be developed in the future. For example, a simple type of IOL might not demonstrate a great extent of accommodation, but might affect pseudoaccommodation. Such an IOL might already exist or there may be a slightly modified version affected by minor changes to the haptics or optics. In any case, further research is required in this field. Another important LAR-related factor is the CCC. A well-centered CCC with an opening of 4 to 5 mm is optimal, as this will help to properly position the LAS with in the capsular sac.
Finally, according to the UBM measurement in this rabbit experiment, it was determined that an LAS 0.3 mm smaller than the IDCP should be used. Some textbooks state that the actual human lens is 0.5 mm smaller than the IDCP, but their recommendations are not definitive as to whether this difference is due to discrepancies between humans and rabbits, or living and dead organisms, or UBM measurement errors. What we know for certain is that accurate and IDCP measurement is critical when deducing results by means of a UBM. A method for accurate and consistent IDCP measurement would position the UBM probe at the spot closest to the center of the cornea, capture as much video from as many angles and directions as possible, and then would determine the IDCP from the largest measurement. Such a method will be especially important to future clinical experiments.
In conclusion, LAS has the potential to maintain a stable IOL position, creating less after-cataract when used in LAR for correction of presbyopia. It can be concluded, moreover, that LAS implantation incurs less damage to the ciliary body. The authors observed IOL stability over a long period of time, and were also able to maintain the shape of the lens angular capsule.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






