


Rhegmatogenous retinal detachment (RRD) can cause vision impairment in certain cases even after anatomically successful surgery. The incidence of RRD ranges from 5.3 to 12.6 cases per 100,000 population [1]. In uncomplicated cases, primary anatomical success rates are generally high [2-4]. Patients who were treated for macula-off RRD might have broad range of visual acuity [5]. It is important to evaluate the preoperative and postoperative parameters that could affect the final functional outcome.
Spectral domain optical coherence tomography (SD-OCT) allows visualizing retinal morphology in detail. In previous studies, the integrity of the ellipsoid zone (EZ) and the external limiting membrane (ELM) and the presence of foveal bulge were associated with the final best-corrected visual acuity (BCVA) [6-11]. The other factors that were associated with postoperative visual outcome were preoperative visual acuity, age, proliferative vitreoretinopathy (PVR), and detachment duration [4,12-14]. However, these prognostic factors demonstrated some differences between studies.
The aim of this study is to evaluate the preoperative clinical and OCT findings that affect postoperative functional and visual improvement at different time points after RRD surgery in a large patient group.
Materials and Methods
Ethics statement
The study was approved by the Medical, Surgical and Drug Research Ethics Committee of Istanbul Medical Faculty, Istanbul University. Informed consent was waived due to the retrospective nature of the study.
Patient selection
Charts of the patients who underwent surgery in the Department of Ophthalmology, Istanbul University Medical School between January 2014 and May 2019 due to macula-off RRD were reviewed retrospectively. Patients who had successful RRD repair, who showed up to regular follow-ups for at least a year after surgery and had SD-OCT (Heidelberg Engineering, Heidelberg, Germany) images at every follow-up were included in the study.
Exclusion criteria included patients with any other ophthalmologic pathology that affects vision, degenerative myopia, nonrhegmatogenous etiology, recurrent retinal detachment, ambient opacities hindering imaging, macula-on RRD, and history of ocular surgeries except cataract surgery.
Protocol
The demographic characteristics of the patients, BCVA, biomicroscopic examination findings, extent of detachment, detachment location, presence of accompanying PVR, vitreous hemorrhage (VH), and SD-OCT characteristics were recorded preoperatively. Surgical methods, duration of symptoms, central macular thickness, presence of subretinal fluid, ELM integrity, EZ integrity, cone interdigitation zone integrity (CIZ), and foveal bulge formation on SD-OCT at 1, 3, 6, 12 months and at last examination were recorded.
BCVA was evaluated with Snellen chart and was converted to logarithm of minimal angle of resolution (log-MAR) equivalent for statistical analysis. Macula-off duration was defined as the time between surgery and onset of subjective complaints (deterioration of visual acuity, visual field defects, photopsia, and floaters). Preoperative ELM integrity was defined as absent, in cases which the integrity could not be evaluated because of folding, undulation, edema, and/or the cases in which ELM continuity was disrupted [7].
To evaluate retinal morphology, horizontal cross-sectional images by SD-OCT at each visit were analyzed. Retinal layers were defined as intact, disrupted (attenuation, discontinuity, or disruption) and absent (total absence of layer) at central fovea. The foveal bulge was defined as an outer segment length at the central fovea being 10 μm longer than the average outer segment length at 250 μm temporal and nasal from the central fovea. OCT images were evaluated by two retina specialists who were blinded to patient’s examinations. Findings that were scored differently by two clinicians were discussed, reevaluated and the final decision was recorded.
Surgical procedure
Twenty-three-gauge pars plana vitrectomy with gas or silicone oil was performed in all patients. Pars plana vitrectomy with additional scleral buckle was indicated in patients with PVR. Patients with visually significant cataracts underwent combined cataract and detachment repair surgery.
Statistical analysis
Statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA) statistics program. Kolmogorov-Smirnov test is used to determine distribution of variables in each group. Independent t-test and one-way analysis of variance tests used to evaluate normally distributed data. For non-normally distributed data, Mann-Whitney U-test and chi-square test were used. A linear regression analysis was used to estimate the relationship between the potential influencing preoperative factors and BCVA at 12 months. In addition, a linear mixed effects regression model was performed to estimate the relationship between the changes of postoperative factors and the changes of BCVA after surgery. For the results, in the 95% confidence interval, p <0.05 was considered statistically significant.
Results
Seventy-five eyes of 75 RRD patients were included in the study. The mean follow-up period was 36.7 ± 16 months (range, 14-72 months). Demographics and clinical features are shown in Table 1. Age, sex, lens status, surgery type, endotamponade type, and silicone oil retention time were not significantly associated with BCVA at 12 months.
Preoperative factors affecting visual acuity
The mean BCVA preoperatively was 1.35 ± 1.24 log-MAR (range, 0-3.7 logMAR), at postoperative 12th month was 0.66 ± 0.50 logMAR (range, 0-1.6 logMAR), and at last follow-up was 0.58 ± 0.50 logMAR (range, 0-1.6 log-MAR). There was a statistically significant increase in BCVA at postoperative 1st, 3rd, 6th, 12th months, and at the last visit compared to preoperative BCVA (all p < 0.001).
Extent of detachment involved one quadrant in 19 patients (25.3%), two quadrants in 34 patients (45.3%), three quadrants in eight patients (10.7%), and four quadrants in 14 patients (18.7%). Mean BCVA of these patients at postoperative 12th month visit was 0.41 ± 0.50, 0.67 ± 0.50, 0.55 ± 0.30, and 0.96 ± 0.40 logMAR, respectively (p = 0.030; post hoc analysis one quadrant detachment vs. four quadrant detachment, p = 0.004).
The mean postoperative BCVA was significantly higher in patients who were operated in the 1st week of their onset of symptoms (mean BCVA at 12 months 0.53 ± 0.50 vs. 0.81 ± 0.50, p = 0.03) (Table 2). Twelve patients (16.0%) had VH and four patients (5.3%) had PVR at preoperative visits. Patients who were found to have PVR in the initial examination had significantly lower preoperative and postoperative BCVA (Table 2). Preoperative OCT images showed that 34 patients (45.3%) had intact baseline ELM. Preoperative ELM integrity was significantly related to postoperative visual outcome at 12 months (p < 0.001). Preoperative factors affecting visual acuity at postoperative 12 months are shown in Table 2.
Postoperative outer retinal changes
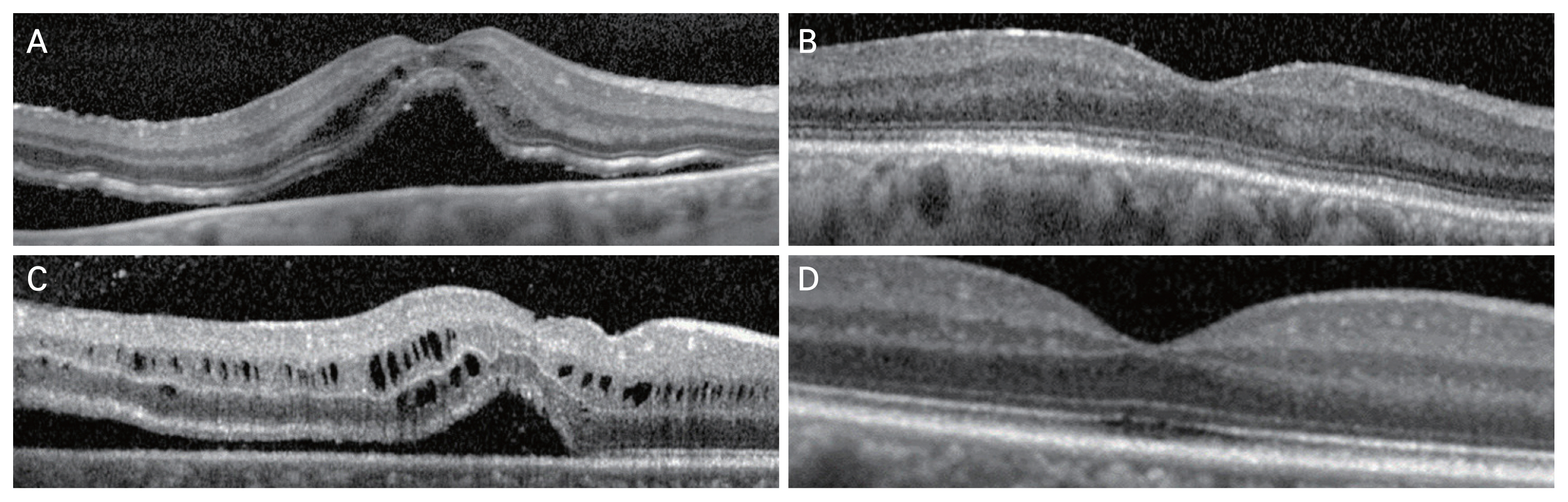
The hierarchical structure in ELM, EZ, and CIZ restoration was observed in our study. The number of patients who had ELM restoration was the highest at 1st month postoperatively and was followed by patients who had EZ and CIZ restoration, respectively (97 intact ELM, 49.3%; 23 intact EZ, 30.6%; 10 intact CIZ, 13.3%) (Table 3). The numbers of patients with restoration of these outer retinal layers consecutively increased during the follow-ups in the 1st year (60 intact ELM at 12 months, 80.0%; 57 intact EZ at 12 months, 76.0%; 25 intact CIZ at 12 months, 33.3%) (Table 3). ELM and EZ were absent in five patients (6.7%) at postoperative 12 months. These patients did not have an improvement in the outer retinal layers at last visit. CIZ restoration in one more patient and foveal bulge restoration in four more patients were seen at last visit after 12 months (Table 3). There was no significant BCVA increase at last visit compared to 12 months (p = 0.26). Preoperative and postoperative images of two cases are shown in Fig. 1A-1D.
Twelve patients (16.0%) were under the age of 35 years, and all retinal layers were restored at postoperative 12 months in these patients. The difference between symptom duration of patients who were under the age of 35 years and above 35 years was not statistically significant (10.6 days vs. 13.1 days, p = 0.38). Epiretinal membrane was observed in four patients (5.3%) at postoperative last visit. Macular subretinal fluid was observed in 13 patients (17.3%) at first postoperative visit and resolved in all patients at follow-ups. Presence of subretinal fluid at 1st month did not significantly alter postoperative BCVA at 12 months (p = 0.74).
In multivariate model, including preoperative and postoperative factors, only preoperative ELM integrity was significantly related to postoperative BCVA at 12 months (Table 4).
Discussion
Anatomical success rates after surgery for RRD are as high as 90%, but unfortunately functional success might be lower in some patients [3,4,7,10]. In this study, we investigated long term results of RRD surgery and preoperative and postoperative factors affecting visual outcome including SD-OCT features. SD-OCT provides in vivo visualization of retinal morphology in the macula with high resolution. It is helpful to monitor outer retinal changes in follow-up of postoperative patients with RRD as it might affect prognosis.
In our study, the mean follow-up period of the patients was 36.7 ± 16.0 months. Similar studies have shorter follow-up periods after surgery [3,11]. This enabled us to evaluate both functional and OCT results for a longer period of time.
In various studies, it was shown that early surgery (within the first 7 days) for retinal detachment has a positive effect on the visual acuity outcome. Kim et al. [15] showed that patients who were operated in 6 days of visual symptom onset had significantly higher postoperative mean BCVA. Williamson et al. [3] also reported that mean postoperative BCVA was higher in patients who were operated in 3 days of symptom onset. Patients who were operated in first 7 days of complaints had significantly higher BCVA at 1st, 3rd, 6th, 12th, and last visit. Similarly, our study demonstrated that early surgical intervention (<7 days) had beneficial effect on postoperative visual acuity. This could be explained by photoreceptor damage in retinal detachment after 7 days. It was shown in histopathological studies that prolonged detachment causes atrophy and apoptosis in photoreceptors [8,10,15,16].
It was previously shown that extent of retinal detachment was associated with postoperative visual acuity. Williamson et al. [3] and Park et al. [7] found a statistically significant difference between the extent of detachment and the final BCVA. In our study, patients with four quadrants of detachment had significantly lower visual acuity at 12 months compared to patients with one quadrant detachment. It has been claimed that vitreous levels of transforming growth factor beta-3 and interleukin-8 were higher in patients with more extensive retinal detachment. Higher levels of inflammatory proteins with a greater detached retinal area indicates an inflammatory reaction due to underlying ischemic conditions and hypoxia which put patients at risk of permanent retinal damage [16-19].
Presence of preoperative VH and/or PVR was a poor prognostic factor for BCVA at 12 months in our study. VH and/or PVR negatively affect regeneration of the outer retinal layers in RRD [3,7,14,20-22]. It has been claimed that this may occur due to some mediators secreted and subretinal gliosis during PVR, affecting photoreceptor healing [23].
In this study, multivariate analysis showed that preoperative ELM integrity was highly related to outcome vision. ELM together with Müller cells forms the connection points in photoreceptors, and maintaining these connections is thought to accelerate photoreceptor healing. ELM damage indicates that retinal damage not only affects photoreceptors, but also spreads to the Müller cell layer [24,25]. Again, duration of macular detachment and extent of detachment affects ELM integrity and restoration [7,8,10,25].
dell’Omo et al. [10] showed that preoperative ELM integrity is strongly associated with postoperative BCVA similar to our results and they observed ELM restoration in first 6 months after surgery. In our study although most of patients had ELM restoration at their postoperative 6 months, we have also seen restoration after this period. Even though anatomical restoration of outer retinal layers was observed even after 12 months, BCVA did not significantly improve after 12 months. Molecular studies are needed in the future to evaluate outer retinal restoration and it is functional effect.
In various studies, postoperative restoration of CIZ, EZ, ELM integrity, and the restoration of foveal bulge positively affected the visual outcome [7-9,11]. Our results were consistent with the literature. ELM, EZ, and CIZ integrity may not be seen in OCT in the postoperative 1st month, but it was found that outer retinal layer could be formed in subsequent examinations. This shows that the regeneration and organization of the retinal layers may occur in the following months. Restoration of retinal layers can be visualized with OCT, and this can be indicator of the functional prognosis.
The hierarchical structure in ELM, EZ, and CIZ restoration was observed in our study. The EZ shows the inner segments, while the CIZ shows the outer segments. In photoreceptor regeneration, first development of the inner segments and then the outer segments were observed [8,9,26]. On the other hand, although the integrity of the outer layers is complete, functional success cannot be achieved in some patients. This may be due to loss of function of photoreceptors. Other cells might replace photoreceptors in the process of healing of outer segments [10].
The integrity of the retinal outer layers in the early postoperative period may be a good indicator of foveal bulge restoration and visual outcome [8,10]. Foveal bulge is thought to occur due to the inner segments of the cones being wider than the outer segments. The restoration of foveal bulge can be associated with the presence of healthy cone cells. Again, the absence of foveal bulge in the postoperative period can be associated with photoreceptor damage [27-32]. In our study foveal bulge restoration improved visual outcome. In the study of Hasegawa et al. [11], at 7 months follow-up, the restoration of foveal bulge was 28.6%. In our study, it was found to be 40% at 6 months follow-up and 48% at 12 months visit. All retinal layers had regenerated at the end of the 1st year in patients less than 35 years of age. The regeneration capacity of retinal layers is considered higher at a young age [33].
The important advantages of our study are the relatively high number of patients and longer postoperative follow-up time compared to similar studies. Preoperative demographic, clinical, imaging, and postoperative OCT findings of relatively high number of patients were evaluated. Limitations of our study included retrospective design and the fact that symptom duration relied on patient recalling. The OCT findings of the patients were examined in a holistic way, only single horizontal images were evaluated, the thickness of isolated retinal layers and the change of these thicknesses during follow-up could not be evaluated. It is known that in a small percentage of cases who underwent retinal tamponade with silicone oil, ganglion cells can suffer a direct damage either from particles of oil that migrate in the retina or from direct contact with silicone [34]. But this toxicity was never clearly associated with visual loss and none of our patients had obvious silicone oil maculopathy or optic neuropathy on exam.
In conclusion, preoperative and postoperative factors can affect functional success in RRD surgery. Retinal outer layer regeneration can continue up to 1 year postoperatively, sometimes even longer. This regeneration especially 1st year postoperatively can be related to better functional outcomes. Preoperative ELM integrity and postoperative ELM restoration are main predictors of functional outcome.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






