

Accurate measurements of axial length (AL), anterior chamber depth (ACD), and corneal power are critical for enhancing the success of vision correction by cataract surgery and refractive surgery. Currently, several devices are being used to measure the anterior segment parameters and AL, including partial coherence interferometry (PCI), optical low-coherence reflectometry, dual or single scheimplug topography, and several types of keratometer.
The IOLMaster 700 (Carl Zeiss Meditec AG, Jena, Germany) is one of a few popularized swept-source optical coherence tomography (SS-OCT)-based optical biometer. IOLMaster 700 can obtain multiple measurements in a single capturing process and presents AL, ACD, lens thickness, central corneal thickness from a single OCT image aligned with the eye's visual axis. The swept source technology provides clear advantages over the partial coherent interferometry that was adopted in IOLMaster 500 (Carl Zeiss Meditec AG, Jena, Germany), including the ability to measure the axial length along six different axes and extremely rapid data acquisition. Moreover, it enables identification of the lens tilt or configuration of the fovea including correct fixation during the measurements.
It is important to know whether the IOLMaster 700 is interchangeable with other conventional devices in clinical practice. Only a few studies have investigated the new SS-OCT-based optical biometer, and they reported the comparison of optical parameters by IOLMaster 700 and only a single device [1,2,3]. The purpose of this study was to compare the measurements in cataractous eyes from IOLMaster 700 with those of multiple conventional devices: OLMaster 500, A-scan (Pacscan 300A; Sonomed Inc., Chicago, IL, USA), Galilei G4 (Ziemer, Port, Switzerland), automated refractor (HRK-8000A; Huvitz, Korea) and manual keratometry(KM-1; Takagi Seiko, Nagano, Japan).
Materials and Methods
Patients
This study was a single-center retrospective systematic chart review of patients who were either diagnosed for the first time or under follow-up for cataracts. Patients who were unable to cooperate and fixate adequately during measurements or had advanced macular problems were not included in this study. This study was conducted at the HanGil Eye Hospital, Incheon, South Korea, between June 2016 and July 2016. The study was approved by the institutional review board of HanGil Eye Hospital (no. 16018) and adhered to the tenets of the Declaration of Helsinki. According to the institutional review board standard operating procedures on retrospective single center clinical study, ethics committee of the HanGil Eye Hospital ruled that subject consent was not required for this study.
Study devices
Biometric measurements were performed as follows: (1) agreement of AL among IOLMaster 700, IOLMaster 500, and A-scan; (2) agreement of ACD among IOLMaster 700, Galilei G4, and A-scan; (3) agreement of white-to-white (WTW) distance between IOLMaster 700 and Galilei G4; and (4) agreement of keratometry-based corneal power between IOLMaster 700 and other devices (Galilei G4, manual keratometry, and automated refractor). The quality control criteria for all devices were applied in accordance with the manufacturers' recommendations. If measurements were not possible in accordance with the limits, they were recorded as measurement failures. A single examiner, who was trained according to the manufacturer's recommendations, performed all the tests. IOLMaster 700 can acquire 7-times AL, ACD, and 3-times keratometry simultaneously for a single report. On the IOLMaster 700, the examiner can see the whole scan image, including the foveal scan for correct fixation.
Device comparison
The IOLMaster 700 was compared to other conventional devices and the results were analyzed to determine the differences for each parameter measured. AL was compared among the IOLMaster 700, IOLMaster 500, and A-scan whereas ACD was compared among the IOLMaster 700, Galilei G4, and A-scan. For keratometry, IOLMaster700 was compared with each of the following devices: IOLMaster 500, Galilei G4, manual keratometry, and automated keratometry. For each measurement, the corneal powers for the flat (Kf) and steep (Ks) meridians were averaged [(Kf + Ks) / 2].
Statistical analysis
The inter-device absolute agreement of each biometric measurement was determined by calculating intraclass correlation coefficients (ICCs) obtained from a 2-way mixed-effect model. Strength of agreement was categorized according to the method proposed by Landis and Koch [4] as follows: 0 = poor, 0 to 0.20 = slight, 0.21 to 0.40 = fair, 0.41 to 0.60 = moderate, 0.61 to 0.80 = substantial, and 0.81 to 1.00 = almost perfect. Agreement between devices was also examined using Bland-Altman analysis, with 95% limits of agreement (LoA = mean difference ┬▒ 1.96 ├Ś standard deviation of the difference). Statistical analyses were performed using R ver. 3.3.1 (R Foundation for Statistical Computing, http://www.R-project.org).
Results
A total of 137 eyes of 78 patients (49 female patients, 63%) with cataractous lenses were evaluated. The mean age of the patients was 66.2 ┬▒ 10.1 years (range, 33 to 86 years). AL measurements were not possible for 10 eyes with moderate to severe cataract using IOLMaster 500, but the IOLMaster 700 was able to measure all eyes.
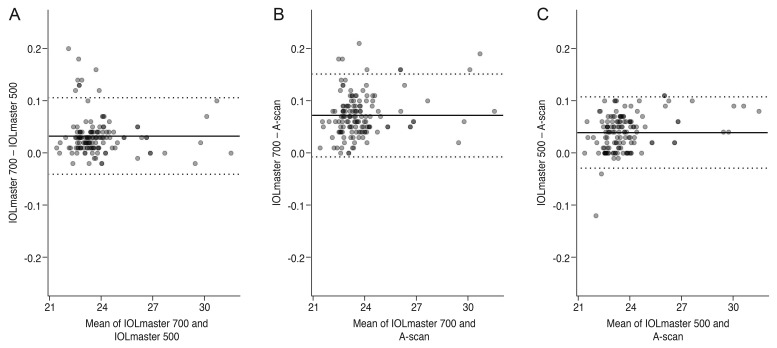
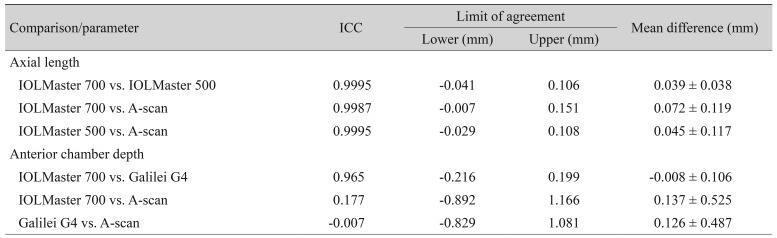
The mean AL value as measured by the IOLMaster 700, IOLMaster 500, and A-scan was 23.82 ┬▒ 1.67 mm (range, 21.42 to 31.53 mm), 23.79 ┬▒ 1.67 mm (range, 21.41 to 31.53 mm), and 23.75 ┬▒ 1.67 mm (range, 21.41 to 31.45 mm), respectively (all ICC >0.99 (Table 1 and Fig. 1A-1C).
The mean difference in ACD between IOLMaster 700 and Galilei G4 was ŌłÆ0.008 mm at 95% LoA (ŌłÆ0.216 to 0.199) with good correlation (ICC = 0.965), whereas A-scan showed poor correlation with the other two devices (Table 1 and Fig. 2A-2C). The mean ACD values as measured by the IOLMaster 700, Galilei G4, and A-scan were 3.16 ┬▒ 0.51 mm (range, 1.65 to 4.67 mm), 3.18 ┬▒ 0.39 mm (range, 1.27 to 4.09 mm), and 3.03 ┬▒ 0.28 mm (range, 2.47 to 3.76 mm), respectively.
The mean difference in WTW distance between IOLMaster 700 and Galilei G4 was 0.029 mm at 95% LoA (range, ŌłÆ0.810 to 0.869 mm; ICC = 0.525). The mean WTW distance as measured by IOLMaster 700 and Galilei G4 was 11.78 ┬▒ 0.47 mm (range, 10.40 to 13.00 mm) and 11.70 ┬▒ 0.42 mm (range, 10.58 to 12.92 mm), respectively.
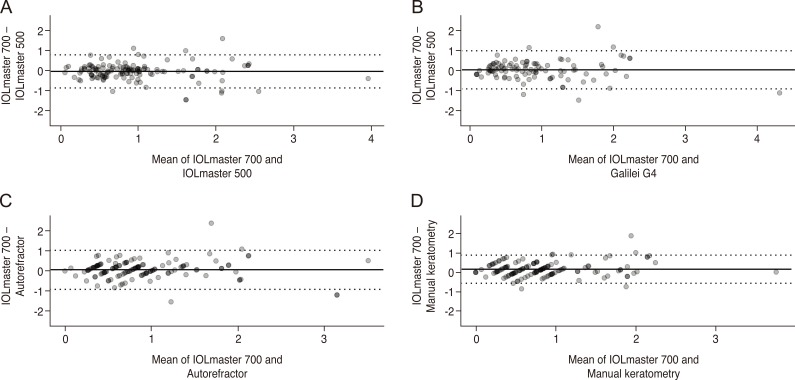
The K measurements of IOLMaster 700 were compared to those of four other instruments (Table 2 and Fig. 3A-3D). Coefficients for the comparison of mean keratometry measured by IOLMaster 700 were ranked 0.989 for IOLMaster 500, 0.984 for manual keratometry, 0.977 for Galilei G4, and 0.936 for the automated refractor. The mean differences in average keratometry for IOLMaster 700 and other devices were as follows: ŌłÆ0.100 diopters (D) at 95% LoA (ŌłÆ0.426 and 0.225) when compared to the IOLMaster 500; ŌłÆ0.045 D at 95% LoA (ŌłÆ0.603 and 0.512) when compared to the Galilei G4; ŌłÆ0.047 D at 95% LoA (ŌłÆ0.486 and 0.391) when compared to manual keratometry; and ŌłÆ0.109 D at 95% LoA (ŌłÆ0.983 and 0.765) when compared to the automated refractor.
The mean cylinder keratometry measured by the IOLMaster 700 was similar to that measured using the other devices (Table 2 and Fig. 4A-4D). The correlation coefficients of the mean cylinder amount measured by IOLMaster 700 were 0.800 for manual keratometry, 0.794 for IOLMaster 500, 0.760 for Galilei G4, and 0.713 for the automated refractor. The mean differences of the mean cylinder keratometry in IOLMaster 700 and other devices were as follows: ŌłÆ0.051 D at 95% LoA (ŌłÆ0.878 and 0.777) when compared to the IOLMaster 500; 0.033 D at 95% LoA (ŌłÆ0.920 and 0.986), when compared to the Galilei G4; ŌłÆ0.158 D at 95% LoA (ŌłÆ0.561 and 0.879) when compared with manual keratometry; and 0.049 D at 95% LoA (ŌłÆ0.923 and 1.022) when compared with the automated refractor.
Although the correlation between IOLMaster 700 and other devices was outstanding for AL, ACD, and mean keratometry, paired t-tests showed statistically significant differences between the measurements.
Discussion
The IOLMaster 700 is the first SS-OCT-based biometry that measures a longitudinal section of the eye (AL, ACD, corneal central thickness, lens thickness) based on SS-OCT with the exception of WTW, which is measured using the light-emitting diode light source according to the iris configuration, and keratometry, which is measured using 2.5-m zone telecentric keratometry (index 1.3375). It provides an image-based measurement, allowing visualization of the longitudinal section of the eye by the measurer. Therefore, it may identify irregular eye geometries such as lens tilt and qualify the image by detection of insufficient fixation during measurements by imaging of the fovea. Furthermore, the IOLMaster 700 was shown to be more effective in obtaining biometric measurements with posterior subcapsular and dense nuclear cataracts than IOLMaster 500 [2].
To our knowledge, this is the first study comparing the new SS-OCT-based optical biometer with five different devices. Rather than assessing repeatability, this study assessed the correlation and conducted paired comparisons between the measurements by IOLMaster 700 and measurements by other existing devices. We suggest that this approach complements the Bland-Altman plots in assessing agreement under a clinical context and leads to a more coherent interpretation of the results between IOLMaster 700 and the other biometry techniques.
Accurate determination of AL is an important factor in intraocular lens power calculations for cataract surgery [5]. In this study, AL obtained with the IOLMaster 700 highly correlated with that obtained by IOLMaster 500 and A-scan. Salouti et al. [6] showed a good correlation between IOLMaster and A-scan, with a mean difference of 0.01 mm. Based on PCI technology, several studies had reported that IOLMaster 700 and IOLMaster 500 showed great correlation with respect to AL measurements [2,7]. These results suggested that both devices measure the AL in nearly the same manner. However, there were eight cases out of LoA that showed higher measurement of AL by IOLMaster 700 than by IOLMasted 500 in the shorter or normal range of mean AL (less than 24 mm). Yang et al. [8] reported discrepancies of AL in myopic eyes but Akman et al. [2] reported there were no discrepancies in any AL. Because there have been few studies comparing the IOLMaster 700 and IOLMaster 500, we cannot deduce the reason for the discrepancy in these cases but it is possible that a small fixation error could occur with IOLMaster 500.
For A-scan, two types of A-mode ultrasound biometry are available: contact biometry and immersion biometry. In immersion-type biometry, which requires placing a saline filled scleral shell between the probe and the eye, corneal indentation is prevented. However, because of the inconvenience of requiring the patient to use the immersion water bath we used contact biometry. Contact ultrasound biometry has been routinely used for a long time; however, the requirement for contact in the patient's fixation makes acquisition of measurements more difficult and corneal applanation might affect the AL values by inducing fluctuations [9,10,11]. Therefore, a skillful examiner is recommended. In our study, a single well-trained examiner performed all the tests, and the correlation of the three devices was excellent.
Our study compared ACD measurements obtained using IOLMaster 700, Galilei G4, and A-scan. The mean ACD measurements from the IOLMaster 700 and Galilei G4 were closely correlated, whereas there was a poor correlation between A-scan and the other two devices. Similar to our study, Galilei had slightly longer ACD values than the IOLMaster, but the difference was clinically very small and closely correlated [12]. The IOLMaster uses a slit beam of light, which is directed at a 30-degree angle into the anterior chamber. Galilei is based on the dual Scheimpflug system principle. Until recently, ACD was measured by A-scan and most studies have found a significantly shorter mean ACD with contact ultrasound biometry than with noncontact optical devices including IOLMaster [13,14,15,16]. This is similar to our results with slightly different degrees. Ultrasound biometry includes inadvertent corneal applanation when using the contact method, which can yield shorter measurements of ACD compared to the non-contact method [13,14,15,16].
The mean difference in the WTW distance between the IOLMaster 700 and Galilei G4 was 0.029 mm at 95% LoA, but the difference was relatively inconstant with a 95% LoA range of 1.7 mm. Differences between the two devices could be related to the differences in digital image processing carried out by each WTW measurement [17]. Devices compare grey-scale steps to detect the limbus point, which lies between the white sclera and the darker iris image, and the corneal diameter is subsequently calculated. As a result, this measurement is affected by anything that induces a degree of darkness during the measurement, for instance an eyelash shadow, nose, or device shadow.
In our study, the range of difference at 95% LoA in keratometry was greatest between the IOLMaster 700 and an automated refractor. We surmise that this may be the result of the smaller diameter at the region measured by the IOLMaster [18]. Keratometric values in IOLMaster 700 and 500 are measured using six light spots in a 2.3- to 2.5-mm radius of the cornea center. An automated refractor and manual keratometry use four light spots in a 3.0- to 3.5-mm area for measurement, whereas Galilei uses a rotating Scheimpflug system in addition to the Placido disk. Several prior studies have reported that keratometric values from IOLMaster 500 were inconstant with those from manual keratometer, automated keratometer, and Scheimpflug system [13,18,19]. The difference in mean keratometry between the IOLMaster and an automated refractor at the 95% LoA range was reported to be 1.20 D by Elbaz et al. [13] and 1.83 D by Whang et al. [18]. When compared with manual keratometry at the 95% LoA range, the difference was 0.45 D in a study by Shirayama et al. [19] and 1.80 D in a study by Whang et al. [18], and when compared with Galilei the difference was reported to be 0.27 D by Shirayama et al. [19]. Although the average differences in keratometry measurements between the devices were compared, it is also important to consider the range of variation in order to gauge the interchangeability of each device.
AL measurements were not possible for 10 eyes with the IOLMaster 500, but the IOLMaster 700 measured in all the patients. This is similar to the results from a previous study in which the IOLMaster 700 was able to measure AL in all 188 phakic eyes while the IOLMaster 500 failed to acquire measurements in 17 eyes with posterior subcapsular or dense cataracts [2]. IOLMaster 700 was able to measure AL, ACD, WTW distance, Kf, and Ks in all eyes within the high-quality standard deviation limits of the manufacturer.
There are several limitations in this study, including its retrospective design. For corrections of astigmatism in cataract surgery with a toric intraocular lens, consistency of astigmatism measurements is mandatory. For a valid comparison of astigmatism, vector analysis as well as degree of astigmatism is needed in order to transform the astigmatism values into the vector components. In addition, subgroup analyses regarding the range of the AL or astigmatism would be needed.
In conclusion, our data suggest that AL, ACD, and average keratometry values of IOLMaster 700 can be used interchangeably with the other devices tested. However, the ACD value between IOLMaster 700 and A-scan and the WTW distance between IOLMaster 700 and Galilei G4 are not interchangeable as the devices have clinical and statistical differences in measurements. In addition, IOLMaster 700 was more effective than IOLMaster 500 in obtaining optical biometry in cases of moderate and severe cataract.



 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






