

Tuberculous meningitis is a chronic disease, and cranial nerve palsies are common manifestations. Neuro-ophthalmic involvement, a part of its presentation spectrum, is important, and numerous reported neuro-ophthalmologic complications are combinations of oculomotor palsies, pupil abnormalities, disc changes suggestive of papillitis, papilledema, or optic atrophy and choroidal tubercles.1 It is always necessary to take tuberculous meningitis into consideration when an abrupt deterioration of a neuro-ophthalmic nature is noted, becauseearly diagnosis and treatment are important. In particular, when a neuro-ophthalmic complication occurs despite anti-tuberculosis therapy, it may be that the tuberculosis is resistant to treatment and that additional anti-tuberculosis therapy is required. The present case report provides an example of rare multiple ophthalmic involvement associated with tuberculous meningitis during anti-tuberculosis therapy.
Case Report
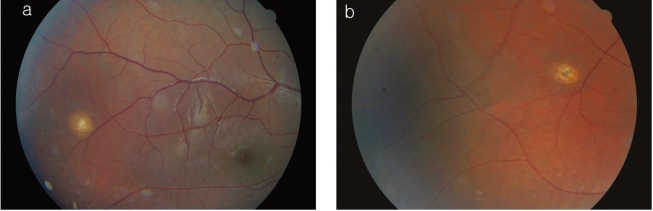
A 15-year-old male visited our hospital for an acute drop of the left eyelid and diplopia of 4 days duration, which developed overnight. One year ago, he was diagnosed as having tuberculous pleurisy (Fig. 1), tuberculous encephalitis (Fig. 2a), and a 2/3 optic disc-sized choroidal tuberculoma (Fig. 3a). At that initial presentation, he had a stuporous mental status. Polymerase chain reaction for mycobacterium tuberculosis on chest pleural biopsy tissue was positive. He was admitted and medicated with anti-tuberculous drugs (isoniazid, rifampin, streptomycin, pyrazinamide, ethambutol) and steroid for 2 months. After anti-tuberculous medication, his mental status became alert and his fever and headache symptoms improved. He was discharged on medication (isoniazid, rifampin) and was followed up in a pediatric clinic without discomfort.
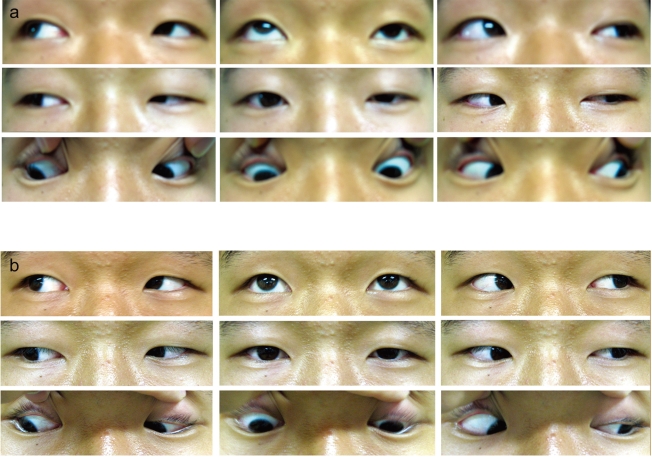
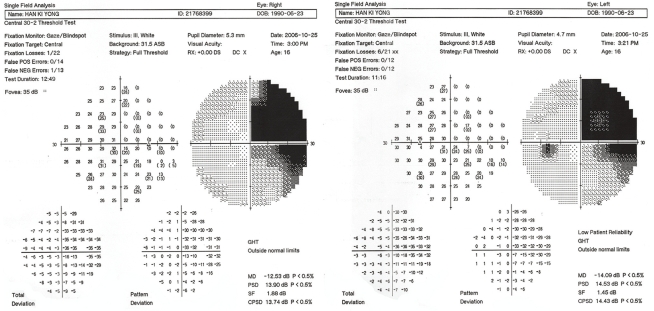
However, subsequently, acute drop of left eyelid occurred and brain MRI showed an increase in the size and number of a multifocal granuloma at the brain base, and increased brain swelling at midbrain and left thalamus (Fig. 2b). He was then re-admitted and a neurological examination revealed a clear conscious patient with isolated left oculomotor nerve palsy, which manifested as ptosis of the left upper eyelid (Marginal reflex distance (MRD) : +4 (OD), -1 (OS), Levator muscle function (LF) : 11 mm (OD), 6 mm (OS)) (Table 1) and paralysis of superior rectus and inferior oblique muscles on the left, but with no apparent papillary defect (Fig. 4a). Other cranial nerves were normal and the uncorrected visual acuity was 20/20 in the right eye and 20/20 in the left. Accordingly, it was suspected that his tuberculosis was resistant to isoniazid and rifampin, and thus, pyrazinamide and ethambutol were added; dexamethasone was also injected to reduce brain swelling. After one month on this medication, no restriction in extraocular movement was apparent (Fig. 4b), his diplopia had also disappeared, and drooping of the left upper eyelid was much improved (MRD: +4 (OD), +3 (OS)). Moreover, the choroidal tuberculous granuloma had reduced slightly to 1/2 the optic disc. After 3 months on this treatment ptosis of the left upper eyelid (MRD: +4 (OD), +2.5 (OS), LF: 15 mm (OD), 11 mm (OS)) improved (Table 2) and the choroidal tuberculous granuloma further decreased (Fig. 3b). However, he complained that he could not see the left eyes of people on television, and thus, visual field testing was conducted (Humphrey field analyzer 2: program C30-2), and a right wedge-shaped sector homonymous visual field defect due to lesions of the left lateral geniculate nucleus (Fig. 5).
Discussion
Tuberculous meningitis is a feared manifestation of tuberculous infection, because it is often difficult to diagnosis, requires a long course of therapy, and is associated with significant morbidity and mortality. Its most common signs and symptoms include fever, headache, changes in mentation, and meningismus in most patients. Other signs include focal neurologic deficits, such as, cranial nerve palsies, paresis, seizures, and diminished cognition.2
Ophthalmic pathologies have also been reported, and its complications include; conjunctivitis, third or sixth nerve palsies, choroidal tuberculoma, homonymous hemianopia, and nystagmus.3 Involvement of the oculomotor nerve can occur due to basal meningitis due to the long course of this nerve in the base of brain, due to vasculitis in the arteries supplying the midbrain region, or due to a tuberculoma situated in the midbrain region.4 Choroidal tuberculoma is the most common ocular manifestation after bacillus dissemination via the blood stream. Choroidal tubercles are frequently unilateral and appear predominantly in the posterior pole as solitary or multiple amelanotic lesions.5 The disease is categorized as follows based on examination findings: Stage1 - fever, malaise, headache without cranial nerve impairment Stage 2 - single cranial nerve impairment due to basilar disease, the presence of paresis and focal seizures Stage 3 - patients are comatose or stuporous and have marked neurologic impairment, including multiple cranial nerve palsies, hemiparesis, or paraplegia this disease stage has a high rate of neurologic sequelae or death despite therapy.2 Moreover, third nerve and optic nerve involvement are also significantly associated with tubercular meningoencephalitis stage 3. Generally, tubercular meningoencephalitis stage 3 is associated with neuro-ophthalmic features, and it is more common in the elderly. This may be because of the better survival ability of older children and therefore a greater chance of wide-ranging involvement. In addition, after sutural fusion at 24 months, increased intracranial pressure is likely to further damage the brain, and in older children aggressive host reactions in the form of basal exudates may further contribute.6 In the present case, due to a stuporous mental status, the patient was diagnosed as having stage 3 disease. Ptosis and external ocular movement limitation due to oculomotor nerve impairment also occurred in this patient. He responded well to treatment, but mild neurologic sequelae remained and he developed another visual field defect. The majority of patients with ocular tuberculosis require systemic therapy, and isoniazid, rifampin, pyrazinamide, ethambutol, and streptomycin are usually administered. Neuro-ophthalmic feature improvements and choroidal tuberculoma involution to a flat inactive scar can occur given accurate rapid diagnosis and treatment. However, neurologic sequelae may remain despite proper therapy in cases of stage 3 tuberculous meningitis. Thus, the prognosis of tuberculous meningitis is related to the timing of the initiation of appropriate therapy. Delays in diagnosis and treatment result in poor prognoses and severe neurological sequelae.
In summary, when a patient with tuberculous meningitis presents with abrupt onset oculomotor nerve palsy, rapid re-diagnosis should be undertaken and proper treatment initiated, because the prognosis is critically dependent on the timing of adequate treatment.




 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






